Madrid area hospitals were forced into wartime-triage, denying care to the elderly in order to give the young a better chance.
By Wisdom Seeker, a WOLF STREET Commenter with a physical sciences Ph.D., San Francisco Bay Area:
This post takes a fresh look at key battlegrounds in the CoronaWar which we discussed last week. For local readers, I’ll take a unique and fresh look at the Bay Area, LA and California. Around the US and globally, Spain joins Italy’s misery, but New York continues to hold out! I share and discuss fresh graphs from a new website, 91-divoc.com by Professor Wade and his crew at U of Illinois.
The graph below all focus on confirmed cases per million population, based primarily on the Johns Hopkins University (JHU) ArcGIS COVID dataset from 3/27, representing cases confirmed mainly through 3/26. California and Bay Area county data were also taken from state and county websites.
These graphs use a log scale on the vertical axis, similar to stock charts. This type of plot turns exponential curves into straight lines, which makes it easier to look at the early behavior and also spot “bending the curve” effects of social distancing and other public health measures.
Two reminders: graphs of “confirmed cases” are subject to limitations and variations in testing. Depending on the level of testing, the actual spread of the disease could be 10-1000 times larger than the confirmed cases. There’s now a “COVID Tracking” website which allows one to dive into the testing details for individual U.S. states.
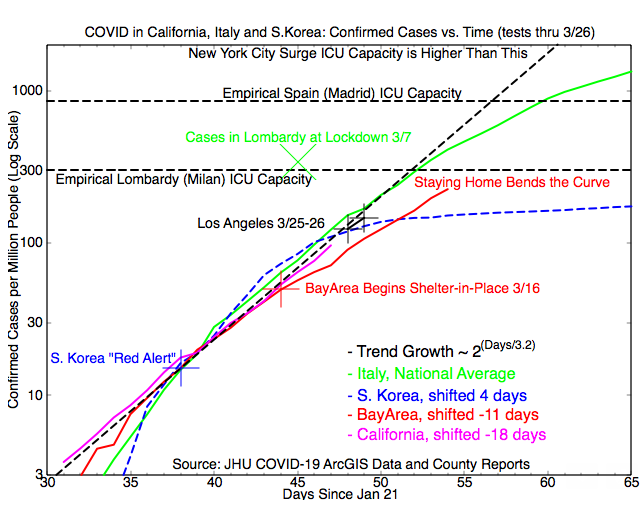
California Hot Spots Compared to Italy and South Korea:
Our first graph this week is an update for California and its two largest metro area hot spots, the San Francisco Bay Area and Los Angeles County. Italy and South Korea are included for contrast: Milan in Italy has been overwhelmed for the past 2-3 weeks and suffered a high death toll, while Korea successfully “bent the curve” so far with extensive test-trace-and-isolate techniques to reduce new infections.
Some good news: The Bay Area has continued to drop off the “Trend Growth” curve, and the effects of the March 16 “shelter in place” are expected to bend the curve further in the coming week, although accelerated testing is hopefully catching a larger share of the total cases. But the Bay Area has overrun the Korean example and appears to be on a curve similar to Italy’s, albeit lower.
By contrast, it looks like LA hasn’t begun to bend the curve yet. As the statewide shelter-in-place kicks in, hopefully that will change!
But, back on the positive side, the “Empirical Lombardy ICU Limit” has proved pessimistic, and I’ve added empirical data for Spain and New York to highlight the range of caseloads at which ICU capacity has held up. More about that below.
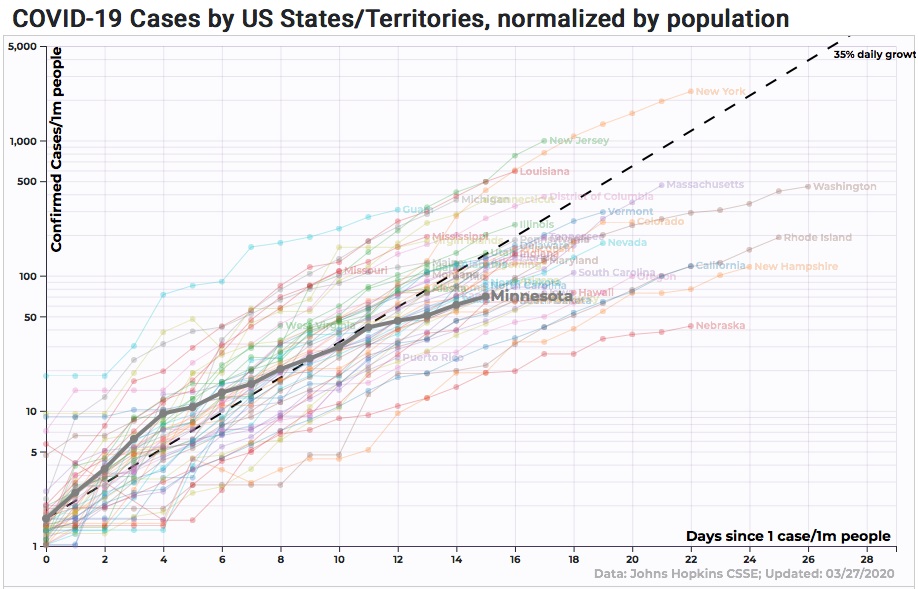
The 50 US States: New York Leads in Growth but Minnesota Bends It Best
Taking advantage of the new 91-DIVOC.com graphing tool, this week’s US State graph features Minnesota, which has exceptionally good testing and appears to be successfully “bending the curve”. Like last week’s plot and the California plot above, today’s graph shows confirmed cases per million population on a log scale. But now all 50 states are included. My one quibble is that the fixed “35% daily growth” trend line appears a bit too steep to my eye.
Among the 50 States, New York sadly holds the lead again this week, followed closely by sidekick New Jersey, and trailed by Louisiana. Louisiana earned my second “COVIDIOT Award” for not canceling Mardi Gras and thereby seeding the whole region with new cases.
New York’s “we don’t need no stinking shutdown” attitude earned them my first “COVIDIOT Award”, failing to account for super-spreading effect of close-quarters living with the nation’s highest population density.
But never underestimate the grit of New Yorkers! So far, they have done better than anywhere at boosting local medical capacity to withstand a huge caseload. New York’s lead, unfortunately, is not simply a matter of more testing: New York has a very high “hit rate,” 30% positive on their tests, indicating that they aren’t testing enough to corral all the cases. I expect New York to have ICU triage issues next week.
By contrast, Minnesota’s “hit rate” is far lower, with under 3% of tests being positive. That’s an order of magnitude lower than New York’s, and comparable to Korea’s. Minnesota also bought time with early school shutdowns, a week ahead the Bay Area relative to the local caseload.
With spread slowed, Minnesota has a chance at “testing out” all contacts of known cases. They might almost corral the virus, and should at least slow its growth substantially. Several other states have also been doing well at slowing the growth rate, but who will be the first to stop it? What does it take?
COVID in the 25 Most Populous Nations: There is Pain in Spain
Last week’s essay highlighted the “most infected” major nations: Italy, Spain, and the “ski nations” of Norway, Iceland, Switzerland and Austria. This week’s graph shifts emphasis to the 25 nations with the highest populations. The US, with the highest number of “acknowledged confirmed” cases, takes 6th place on this graph “per million people.”
Spain and Italy are at the top of the curve again. There is heartrending pain in Spain this week: Madrid area hospitals were forced into wartime-triage, denying care to the elderly in order to give the young a better chance. Wuhan, Iran, Milan, Madrid – who will be next? The next three contenders are Paris, New York, or a hot spot in Germany.
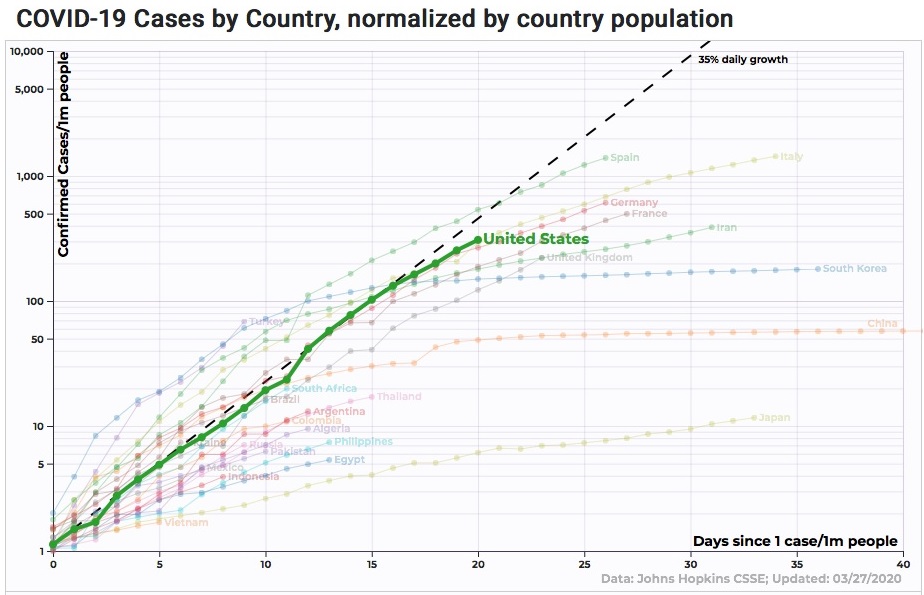
One last comment – nearly hidden on the left of the chart is the purple curve for Turkey, which has just overtaken China for 9th place. It’s good to see Turkey “catching up” in testing, but the data indicate a large underlying infection level. And amidst a pandemic, Turkey’s move this month to export 4 million refugees becomes a grave concern for the whole region.
On the positive side, many nations have begun to “bend the curve” and shift to slower growth rates. Let’s hope that continues! By Wisdom Seeker, for WOLF STREET.
Enjoy reading WOLF STREET and want to support it? You can donate. I appreciate it immensely. Click on the mug to find out how:

![]()
One of the most unsettling side effects of this virus is that when someone in your family would wind up in an ICU-bed dying, you could not even be with them and support/accompany them in their final moments. We live right next to my 90 year old parents-in-law, my own parents are now 82 and 89 repectively. If one of them would catch it, I would have to say goodbye from a distance. Heartbreaking stuff.
Similar situation here. Are you taking any special actions as a result of the situation? Over here we’re all hoping for the best, but realizing that there’s never going to be a better time to talk often, repair relationships where needed, and make sure we have a plan if someone does get a bad case. If it does get bad, people won’t be able to sit at someone’s bedside and fill out the various medical / legal / financial forms at the last minute.
Only one possible solution for it for now: we avoid all contact with the four parents, don’t come in their houses, they are only to leave their homes to go into their own garden, we have sort of ordered them to stay put until the all clear will be given. We take care of their groceries/errands to the pharmacy and leave the stuff at their doorstep, then give them a call to pick it up. No contacts whatsoever with us or the grandkids unless through the phone, over the hedge or in case of an emergency. For instance, last week I had to go and pick my father-in-law off the floor at night, when he had fallen out of his bed and couldn’t get up anymore. Sounds a bit like a slapstick now, but at that moment I was thinking: Jesus, I have to get him into his bed asap, breathe as little as possible while doing so and then get the hell out of their house.
Yeah, it gets tough. In situations like that, I think there are some simple steps anyone can take to reduce risk a little and, perhaps more importantly, buy a little peace of mind:
1) Wear any kind of face covering you have, and any gloves you have, whenever you need to interact. Not as good as an N95 but anything is better than nothing. And a trip through the laundry dryer afterwards will kill the virus so you can reuse. Saves the N95s and surgical gear for the hospitals, but still protects family.
BTW, this topic is featured in _Science_ today, the top US scientific journal.
2) Quarantine treatment for groceries (and mail). Handle stuff with gloves until treated. Safely stash non-perishables to sit for a few days; the virus dies off fairly fast on cardboard and paper and such. Where possible, perishable items get a wipe-down with a soapy towel or a disinfecting wipe. And don’t eat right away.
Two attitudes that make this sort of thinking flow naturally:
A) Focus on keeping the home safe, so you treat everyone and everything from the outside as potentially infected until it’s been thru de-con of some kind.
B) Assume that you will get caught up in a contact-trace at some point, because of exposure to a confirmed case. And you don’t want to be embarrassed by your own contacts, who suddenly become “people whose lives you might have ruined” if you too got infected.
It’s a cold and harsh reality, but these could help to keep more people alive.
Lost my father in law Wednesday, age 93+, not from this virus, but still not happy; he was a good man, hero of WW2 and Korea, and VA took great care of him. Nursing home moved him to special room so his kids could be with him at the end, after they were temp tested to get in the place.
So do your best and then you just have to let go and let God (or your version of the Great Spirits,) take over.
Excellent suggestions WS, I really hope folks will follow them as much as possible:::: and good summary of the situations. Thank you.
Meanwhile, we must all understand that this virus is mutating fast; 5 known ”clades” Thursday, and LH said yesterday that there were 10 clades and at least 100 sub-clades as of then, maybe a lot more per ER doc,, so really fast moving.
And that means, at this point, the ONLY effective means of slowing it down is STAY HOME!!
VVN,
But are the mutations you cite more dangerous, less dangerous, or irrelevant?
Mutation will have implications for vaccine development if the are equally or more dangerous…otherwise I’m not sure if they are negative per se.
If you think about what tiny genetic fragments viruses are (so stripped down they need others’ cells to reproduce) and the vast replications they go through in a single body…and how many bodies they pass through, a high rate of mutation may not be that surprising.
Like so many discussion pts surrounding C19, there seems to be a huge demand for contextual information.
WS
This is a tour de force, some of the best and most insightful analysis I have seen. Thanks.
The world in data website also has some similar data searchable by country, including daily death rates, which are probably the most accurate measure, as testing is too variable between countries.
Don’t let that thought trouble you
I have been near death a few times, and quite frankly no company could have made it any better.
In fact, I would much rather get on with it on my own, and spare others any distress.
Especially in the case of something infectious.
At least they had time to grow old and form a family and even have grandkids.
Any small kid under five can easily die of Coronavirus, more so if they have any kind of previous health problem.
Small children, old people over sixty and people with pre existing health problems are more at risk but this disease has already killed people that wasn’t in those groups.
So literally anyone can die from this disease.
The CCP Coronavirus isn’t a significant risk to little kids or teens. Possibly a couple of kids under 10 have died from the coronavirus, but, it’s actually less dangerous than the usual flu for them specifically. It’s very unusual for a virus, but this virus is less dangerous to infants than the general population. Overall, for little kids, I wouldn’t worry at all, everyday things are far more dangerous to them.
For teens and people in their 20s the risk is slightly higher, but unless you have a medical condition, are substantially obese or something similar the risk is near zero “there is also a few unlucky random ones”. Other things are just as dangerous. Because, it’s been spreading faster among the 20s and 30s they have been disproportionately represented in the hospital.
You do realize that your point about “disproportionately represented in the hospital” contradicts your “risk is near zero for teens and 20-somethings” claim? If the risk was negligible they wouldn’t be showing up en masse in hospitals. Because they don’t for anything else.
We’re going to hit the point soon, starting in NYC where every hospital bed taken up by anyone, is a bed denied to someone else who needs it and is therefore likely to die.
The fatality rate for 20-somethings will remain low b/c they will get priority for ICUs (under triage rules), but they will be costing older people their lives.
Notice that I mentioned kids aged five or younger not kinds under 10.
raxadian,
All kids including those under 5 have essentially no risk. Across the entire World, some under 5 will die, but far less will die “kids under 5” from the coronavirus than many other things. Sids, car accidents, and many other things will probably kill more. Even the couple of babies that died so far, may have died from other things, in particular the first baby who died in Wuhan had other more serious health problems.
Wisdom Seeker,
I didn’t say teens were disproportionately in the hospital, I said people in their 20’s and 30’s “this also only applies to some hospitals”. People under 40 make up majority of the populations in most countries as well.
The actual data in the wild about how whose affected is terrible “except South Korea, I think”. We mainly are getting anecdotal data like, many of those in the hospital are under 40. This is a dumb thing to not clarify. Are most of them late 30’s? Younger?
In general in most cities in America, people in their 20’s “and 30’s to a lesser extent” make up a large proportion of those in retail, restaurants, and other general public facing jobs, they are also the ones most likely to travel around alot. They will typically be the ones to first get it and spread it around. In many cities for instance, after they got infected, even if it wasn’t serious many cities might have automatically admitted to the hospital, everyone with the coronavirus, how widespread would this be??? Just saying who’s in the hospital doesn’t tell us alot, it would be more useful to know who’s going to the ICU. We’ve only got anecdotal data for that.
All of this also doesn’t tell us what percent are infected, immune, asymptomatic or only experiencing mild symptoms.
To actually deal with the crisis, the CDC if it isn’t already “I don’t think it is” should be collecting all data on every single patient. And instead of focusing on making ventilators “they still should, but right now, they are doing this and are acting like that’s enough”, should be asking for volunteers from those who get the coronavirus, who are willing to be a guinea pig to test all the possible anti-viral and other medications. We should be focusing much more heavily on production of those treatments that prove effective, those treatments will prevent the virus from progressing far enough that hospitals will get overwhelmed as much. Administering medications en masse, should be much more possible, then putting millions on ventilators.
In general, to actually understand whose affected and how much, I would only trust the South Korean data.
Indeed anyone. Italy reported more then 50 docters have died by C19.
Definitely. My best wishes to you and your family. Those of us with children also have to worry that if we see our elderly relatives, since kids are often unknowing carriers, we might inadvertently carry the virus to them that might ultimately kill them.
Large buildings, like so many in New York, may magnify some outbreaks. One danger is what happened in Hong Kong during the SARs outbreak. See https://www.ncbi.nlm.nih.gov/pubmed/16696450
There were buildings there that had massive outbreaks. Seehttps://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=4&cad=rja&uact=8&ved=2ahUKEwjF4IqQvr7oAhXPIzQIHRoWB1IQFjADegQIBxAB&url=https%3A%2F%2Fwww.livescience.com%2Fcoronavirus-can-spread-as-an-aerosol.html&usg=AOvVaw0hqJVDdJPXnZCpj3fiI6N6. There are theories.
However, it is not truly definite whether this was from plumbing or the common ventilation shafts shared by the apartments carrying the virus or bathrooms, elevators or elevator buttons or other common areas, e.g., lobbies, which had things that were touched by tenants. If I was going to rent today, I would try to avoid any such huge, interconnected buildings, which have gotten more and popular in LA and OC.
I presume that they are great for singles to meet each other: with common pools, exercise rooms, etc. However, even those buildings’ chances of surviving an earthquake are reportedly less: wood has a certain level of compressibility and elasticity. Those buildings are so huge and heavy, and have interconnections, that their wooden structure might be closer to its limits than in a smaller building.
I must definitely hope that history does not repeat itself. I guess that there are much fewer shared, community bathrooms among residents in NY buildings, so let us hope that will change the spread of the virus in those buildings.
Masks
I agree.
But can you get them?
Seems to be a worldwide shortage.
Very hard to get in my country.
Military Personel came to a friends panel shop and bought all the masks they use when spray painting.
PPG has been rounding up every paint shop mask they can find nationwide for contribution to the effort.
You don’t need a medical-grade mask to slow the spread. Any face covering helps. Improvise and add some style!
FANTASTIC. Finally, a website that gives actual data + some qualification of how good the data is.
The only thing I could ask for is 3 trend graphs (deaths, recoveries, cumulative cases) by state. I know aggregating large geographic areas somewhat scrambles the data, but everybody is looking for some indication that he massive changes in our collective lives is actually achieving what we’re all hoping for (flattening the curve).
Hi Javert – Recoveries are really hard to measure and not well reported. Even deaths can be problematic in the hardest hit areas – treatment takes priority over testing. Bay Area is likely to have enough deaths (sadly) that a graph of deaths overlaid with confirmed would be meaningful next week. Maybe New York too. If I get some time and it works out, I’ll share.
I finally figured it out – great functionality in the charts.
On the ground report from MN. We have not had access to many test kits until recently. Around these parts, we are more or less stuck indoors for many winter months. I have been out on remote walking paths every day for the last few months, even on single degree weather, being I have a new
puppy. Everybody has been keeping a social distance even before our current mandatory two week shutdown that began today. The MN Nice thing is actually real. I keep coming across positive messages written in chalk on walking paths in the last week.
MN is NOT testing unless someone is critical and needs to be hospitalized. The numbers are skewed. I live in the cities. U of M has 16 positive healthcare workers. 750 + self quarantining who wont get tested. So give MN a few weeks. Its coming.
Another anecdote from MN. People here are rule followers, and in the best of circumstances aren’t more than superficially friendly – so not hugging or shaking hands or going to each other’s houses is not a heavy lift. Also, the weather has been dreadful, so not a lot of incentive to leave the house. That said, tests have NOT been widely available except for a few days when they were first available – about 10 days ago. Very quickly we heard that testing was only for the very ill. I had one friend whose test took a week, and heard second hand about one that took 13 days! So it’s a mixed bag. Fingers crossed the curve continues to bend.
Worldwide waves of infection and reinfection will be in flux as rules on social distancing and travel are updated. This will occur as local economies crater. Eventually an antibody test and shot will be available.
You are a real piece of work. Like Tom Stone, I wish you would voluntarily refrain from commenting on this website.
Michael Engel :Please try to get Donald or Joe to answer this and put it up on you tube. I need some entertainment.
It doesn’t surprise me that MN is doing well. The people there are more community-minded than the average American and think more about the impact they have on others.
However, it is not without sad COVID stories. Senator Klobuchar’s husband is on oxygen after being infected with the virus.
Minnesota is still in Winter, but outside Minneapolis/St.Paul, is very rural. Not surprise to see them doing well.
YW,
The seasonal/temperature highlight is well taken.
One thing about cold Temp (typically thought to worsen flus, etc) is that it tends to encourage self-isolation – few people like running around when it is freezing outside. A lot of people hunker down indoors, by themselves or with immediate family.
MSP hit 60 F yesterday, and in there were tons of people outside during dinnertime.
MC01: Tuono means thunder in Italian (which, of course you know, but I just learned). Damn, I love my thunder!
DR,
If temp spiked and crowds gathered, it will be interesting to see if cases spike in the next week.
If so…that may be an object lesson for other metros.
If not, perhaps an indication that C19 has seasonality.
For the most part, people were only next to each other’s spouse or kids. A safe distance was kept between others very well and orderly.
As I commented yesterday, Minneapolis has shut down some parkway streets to motor vehicles to give pedestrians, runners and cyclists extra room. There are biking and walking paths around the lakes, Minnehaha creek and the river with a lot of room to keep a distance from anyone else.
Mid 40s F and drizzly today; not too many outside but us regulars at mid-day.
“to give pedestrians, runners and cyclists extra room.”
I understand the impulse (though it has only been about 10 days)…but the Asian countries look at us and think we are f*cking nuts to loosen lockdown so quickly, for what seem such trivial reasons.
Ditto the attitude on masks and gloves.
At least quicker reporting is getting in place, so cause-and-effect will be more definitive in terms of actions taken and results obtained.
Hopefully it won’t be a lesson learned in blood.
Oops Wolf you deleted Michael’s comment. You can delete my response now thanks.
Adding New York city curve to the first chart would be a good comparison to the Bay Area.
New York times did a curve comparisons chart by state and country.
https://www.nytimes.com/interactive/2020/03/21/upshot/coronavirus-deaths-by-country.html
DC area is still around ~2000 cases. Most of the people stay inside. I think they are testing enough people. MD alone tested more than 11,000. In grocery stores, only a few are wearing gloves and masks, follow the six feet distancing. Otherwise, its pretty calm out here. I hope everything comes back to normal by summer.
Personally, I don’t get the hesitancy to wear mask and gloves – assuming personal supply (and passable glove improvisation appears simple, even plastic grocery bags themselves can be wrapped and tied off around hands).
(I am not talking about m/g as a substitute for isolation/distancing…but some grocery trips are going to be a reality for many/most for a long time…so the m/g issue remains important)
The near universal distinguishing trait between Asian and western populations on video is the wearing of masks…and most Asian nations have done better than most western nations.
There have been gvt mixed messages (with mixed motives) on various mask types in the west…but the better performing Asian nations just seem to go ahead any wear them – whatever kind is available. (No need to get into a std vs N95 debate here…Asian nations seem to go ahead and use whatever is available)
In the west – a lot of debate as to effectiveness (with some con positions seeming inconsistent)…but since there does not seem to be a lot of downside to wearing gloves/masks (except in very specific circumstances) why not default to using them?
Embarrassment maybe…but alternative seems much, much worse.
We’re starting to get over the face-cover-and-gloves stigmatism.
I predict that gloves will be back in style like in the Victorian era. I suppose face coverings will be the new top hats!
We’re starting to get over the face-cover-and-gloves stigmatism.
Yes, we are truly turning Japanese. This is something that has been mentioned on this blog several times.
Anti-maskers are this year’s anti-vaxxers. Cover up!
Handwashing is far more effective than a surgical mask and is the most important factor in spread for this disease. Masked people are typically also handwashing, but the mask wearing behavior you observe in Asia is largely cultural and not based on sound principles of disease prevention unless you are near coughing people.
That’s not strictly true….wearing masks make you much less likely to pass the virus on and that is why wearing masks is such a good idea, especially as the virus can easily be spread by something as simple as breathing out, more so if you are indoors in a supermarket , for example….
Retail establishments like grocery stores are beginning to erect plastic “shields” between cashiers and customers…..
Trader Joe’s as some others are doing only allow a certain number of customers into their stores at any one time.
Yesterday I was out procuring food items at various stores, when while shopping at the local ‘organic’ grocer, I found myself transacting my purchases in front of a rather large clear ‘deflector screen’. It seemed to work somewhat as an unintended wall of silence, blocking sound transmission between customer and cashier … whereby vocalizations had to be increased on the intensity scale from say 6 .. to 10.5 (just below Spinal Tap threashold!!) between parties as a result on said saftey ‘barrier’.
Just one aspect of Life in the time of Corona …
Just read that Michigan added 1000 cases overnight. Vast majority in Metro Detroit with city of Detroit 80% of total. Mayor Mike Duggan, a white mayor in a almost entirely black city, usually treads lightly, blasted his constituents for still engaging in large gatherings and ignoring social distancing. My daughters both work in local hospitals in the suburbs and will be in danger due to the hospitals filling up with city residents who don’t give a crap.
Another factor may be “lumpiness” in testing/test result returns.
If you review the day by day, state by state results, it is not uncommon to see very odd stagnation/spiking of numbers on immediately successive days.
I think those may be more the result of data collection/reporting discontinuities than anything the disease may be doing.
Ditto for adverse selection in the now faster testing of numerous backlogged testing candidates…methodological artifacts can cause unusual results for a while.
It averages out over a few or more days…but the sudden spikes can cause a lot of consternation when used to base projections.
Indeed. Real world data is always messy compared to those beautiful models and simulations and video games…
“Wuhan, Iran, Milan, Madrid – who will be next? The next three contenders are Paris, New York, or a hot spot in Germany.”
Germany has by far the best response in Western Europe. You take the wrong indicator. Confirmed cases depend on the number of test performed. Germany has a 500k test capacity per week. The UK aims for 70k. In Western European countries outside Germany and Austria you better look at the death rate per day and its momentum. You can do so at this website:
https://covid19info.live/
The next big hotspot will be in the UK. Deaths there are soaring at an extreme rate. Yesterday UK had 260 dead people, the day before 180 and before that 115. A death rate of more than 5% in the UK simply means, that most infected aren’t tested. The current death rate in Germany (dead/positively tested) is about 0.7%. Due to the early testing, the death continues to climb after the positive test rate is leveling off. But due to the high test rate, I’m confident, that the plateauing in the positive test rate will soon as well transform into the same for the daily death rate.
how you cone to the conclusion that germany has the best response puzzles me a bit
i live in germany in obe of the hardest hit regions with a lot of industry.
nobody is taking this seriously. bot the politicians (similar thoughts like in the us are expressed already after not even a week of “quarantine” ) people still go to work. factories are open. most shops are closed. many are still open. yesterday 28 march the local hardware store was open also a furniture store.
traffic is almost the same.
people still go work. you are not allowed to meet more than two people but still must go to work with hundreds of others.
great response.
state employees still going around and working as if there is no crisis.
germany has a great pr machine and knows how to sell itself.
i predict a bad outcome for germany.
Thanks for the update on Germany! I see what you’re saying about testing, and catching the confirmed cases early could help to slow the spread. But I would note that the rate of growth of deaths in Germany (1.26x/day for past 6 days) is about the same as in the UK (1.23x/day for past 7 days; 1.30x/day for past 10 days). So Germany is only a week behind UK, France and Switzerland in terms of deaths per capita.
Some informations from Italy, we are now where some places in the US will be in 2-3 weeks. First, statistics are mostly noise in the early stage, number of cases the less informative of all. There are only two numbers to monitor closely, deaths and above all patients going in and out ICU. The very sick requires a very long period in hospital, 3 weeks, sometimes more. So it’s a queue problem. The number of people going in is 100 times higher than people going out at the beginning of the epidemic, where NY is now. So a city as big as NY needs a huge number of ICU beds. Second and very sad, the number of deaths from Covid-19 will be much higher than reported. That’s because old people will die alone at home or in nursing homes that are at maximum risk. There were many cases here and other in Spain. It will happen in the US, UK and everywhere. A rough esteem was made comparing the number of deaths in the same period for 2019 and 2020 in some small towns close to Bergamo and Brescia and it is up to ten times the normal and only a small fraction will be labeled as death from corona virus. There are no people, no swabs to spare for them. It’s extremely sad but it’s happening. Also, some form of triage will be applied or already is. It will be hard. Be emotionally prepared and strong. US has a younger population, this helps but a lot more people overweight and this is bad. Another very disturbing thing is this: in Italy we have one huge outbreak but many other, albeit smaller, in other regions at a different stage. The bigger the country the worst under this aspect. This means that even when the main outbreak will be under control it will take a lot of time to be back as normal. There are also some good news coming. As expected the fastest area where solutions have benn found is diagnostic; Abbot Labs announced a fast test equipment to be produced in the millions. I believe this a game changer for prevention and controlling future outbreaks. Therapies will take time, too much for the outbreaks running now. Vaccine is very far, I’m personally connected with specialists and they don’t believe a reliable one will be ready to be massively produced and distributed before 18 – 24 months but there is no guarantee at all, RNA viruses are tricky because of fast mutations. That’s also what Novartis says and I believe more in big pharma than some small bio start up with little or none history. So now it’s all about placing all the efforts in containment. In the early stage with a 33% daily increase, an hour less saves many lives. Good luck and be calm, it will pass.
The parade of unknown, investor-fishing, companies promising miracle rapid and safe vaccines in a few months is, frankly, utterly tasteless.
Improved diagnostic capability is vital: then we can have intelligent and measured containment and management policies that do not crash economies, and drive whole societies mad with confinement and lack of exercise.
And, above all, in the meantime people need to wear masks, gloves, and avoid exposing their hair.
Thanks Francesco, but people in the US have been told that it’s ‘totally under control’ and they’ll be able to start going back to work in a few days. Ha sempre ragione.
There was a similar campaign in Italy a few weeks ago – #MilanWillNotStop, which the mayor of Milan even joined in.
Then the hospitals overflowed and the bodies piled up. The mayor now admits that what he did was “probably” a mistake (?!)
In Brazil, Bolsonaro, has started a similar campaign #BrazilWillNotStop”.
I think we know how that story will end
Now now Gandalf, we do not point fingers at political figures on this site, regardless of how richly they deserve removal from office or how much blood they end up having on their hands.
Once upon a time we were also told we had “nothing to fear, but fear itself”, and that wasn’t true either. The point isn’t to tell a perfect truth, but to help steer the public mind in a positive direction and avoid further mass panic. And it has been working. People in lockdown are much more productively employed working out how to get out of lockdown (without dying) than wallowing in misery.
The point isn’t to tell a perfect truth, but to help steer the public mind in a positive direction and avoid further mass panic. And it has been working.
It’s been working so well that the mortality projections go up every time there’s a national cov-19 press conference.
Francesco, thank you for this extremely valuable information! I am impressed that some parts of Italy have already worked out “excess mortality” information. If you have a link to any of that, I would love to see it. I have access to Italian translation. I hope it is mostly over for the early-hit towns now?
You are right that deaths from confirmed cases will never tell the full story. Overall excess deaths (compared to normal levels) will be far higher. Sadly, that data never came from Wuhan (so far as I know) and would have been the most important of all. No doubt not flattering to CCP though.
I also hope the US and other nations get around to systematically reporting ICU levels. One can do estimates from confirmed cases (or from deaths) and see where ICUs fill up, as I have done in the first figure here.
But if we had a graph of known ICU capacity (hopefully expanding as surge measures roll in) and compared it with growth in ICU usage, that would be far more directly informative. The slow resolution of COVID requiring long ICU stays is going to be a huge issue for those infected who need hospital care later on.
“Slow resolution”
That is a big, big reason why absolute ventilator numbers may need to be so high…the resolution phase (for either good or bad outcomes) can extend into the weeks, meaning that simultaneous demand can be very high, limiting reuse, and maximizing the absolute numbers needed.
That is why I wish I was seeing more alternative oxygenation modalities proposed (short of ventilation)…even merely delaying the time-to-ventilator can have significant impacts upon peak simultaneous ventilator demand.
Yes. I wonder if oxygen concentrators are still available on Amazon for $1500 each? Those could be very valuable.
WS,
Simple patient positioning can sometimes help oxygenation (at home or in the hospital) at least for a period of time…and yet there is almost zero coverage of something that is accessible to all, immediately.
And I believe there are drugs that can assist with pre-V oxygenation…but again very, very little public discussion.
Perhaps these drugs are being used, but considering that the same pts get hashed, and rehashed, and re-rehashed on cable, it would seem more productive to cover every phase of the disease process in some detail.
The networks have made explicit autopsy procedurals a thing over the last twenty yrs…why shy from discussing much, much less graphic medical details?
Instead of practical knowledge we are given political warfare.
There are some means of alternative oxygen provision, but they are far inferior to mechanical ventilation, which is why they are only used in times like these when there are no other options.
Re “Depending on the level of testing, the actual spread of the disease could be 10-1000 times larger than the confirmed cases.”, that seems intuitively true… and would mean the actual mortality rate is 10-1000 times lower. Nobody seems to get that.
Still, 10-1000 is a very big range… have you been able to find any published data or analysis to support or narrow down the number of active cases. I can’t understand why we are not doing widespread random testing to find out – that’s the trillion dollar question!
NicC – it doesn’t mean the mortality rate is lower, because those other 10-1000 cases haven’t resolved yet. Typical confirmed cases are deep into the progression of the disease, have symptoms, are maybe in the hospital, and had a couple days lag to get the test results. In the 1-2 weeks between when that person was infected (along with others who never got tested yet) and when they got their test results, many other cases have sprouted up but just haven’t hit full fever-bloom yet.
A little off topic. Was talking to my GM engineering brother in Detroit last night.
GM & Ford are both making face masks. They have everything except the face mask fabric.
The problem everyone in the US faces is the fabric to make face masks is only made in China and China is not allowing any fabric to be exported.
The solution is to have an auto sound deadening material supplier in South Carolina tweak their sound deadening material density, this weekend, down from 75% to the 25% required to make this face mask fabric.
By adjusting their machinery, this auto supplier will be able to produce 1 million square yards of polypropylene spun face mask material by this coming Friday.
This will allow both GM & Ford to ramp up face mask production shortly.
Regarding GM making ventilators.
In the last 2 to 3 weeks GM production engineers have been able to source all of the over 700 parts needed to make ventilators.
The ventilators will be made in Kokomo, Indiana, by what we used to know as Delco Electronics, GM’s radio supplier. Production will start late this week and will quickly gear up to 1,000 ventilators per day.
So at least some good news for Americans!
The sad news is up here in Ontario, the government is only now removing the restrictions placed upon private companies to help fight the virus!
I get the focus on ventilators – they are the consensus endpt treatment of C19 progression from infection to pneumonia to hospitalization to oxygenation to ventilator.
And I realize that they are the resource intensive bottleneck (albeit at nearly the end of the progression) – so more power to those working hard to accelerate a complicated process (and even more power to the MIT and Rice engineering teams that have kludged together working prototypes of low resource, low cost, scalable ventilators…hopefully some mass production firm has tied in with them).
But that said, I wish I was reading more about (perhaps non-std, but reasonable) treatments (mostly drugs) aimed at reducing/slowing the progression of steps at a more intermediate stage.
The thing to keep in mind is that the consensus treatments at all stages is currently yielding the dangerously accelerated need for ventilators…slow the intermediate steps, and the demand curve for ventilators slows.
Obviously there are a lot of proposed drug treatments for front end C19 infection (to me, the repurposed meds suggested by translational medicine experts make the most sense…they have all been through the long process of safety testing…it is only their C19 efficacy that is unknown, but which can be computationally modeled very quickly and then rushed to efficacy trials).
But I have heard very very little concerning other intermediate steps (defense in depth tries to address every intermediate step in a progression).
Take oxygenation for example. It would seem to me there must be multiple drugs/therapies that increase blood oxygenation…delaying (or maybe even eliminating) the time-to-ventilator.
By definition, these approaches would be non-consensus…but since the consensus trmt pattern is yielding the unacceptable acceleration of ventilator need, I am puzzled by the lack of inquiry into these alternate modalities at earlier stages of progression.
If GM/Ford can deliver a reliable mass product in a compressed timeline wonderful (but in which case they would be Toyota…and not the outperformed GM/Ford of recent decades).
I hope they pull it off…but putting too much exclusive focus there may be a mistake.
I get the focus on ventilators
The governor of NY asked for 40,000 and was told by the Expert In Chief that “I don’t believe you need 40,000 or 30,000 ventilators.”
But I’m glad you get it, cas, but there seems to be a difference of opinion here. How many do you believe NY might need?
I believe the end number is uncertain, but that the conservative approach is to assume the worst – consistent with the limited resource and the potential need of 49 other states.
There are intermediate steps that could be taken with the limited national stockpile – for one, a greater number (but not all) could be moved closer to “peaking” areas so that delivery times are minimized…as demand is actually realized and not simply projected.
Projections are always going to be very, very sensitive to the assumed initial variables – which in the real world, fluctuate a lot from day to day. The NY doubling rate changes significantly from day to day – watching the daily C pressers highlights that.
Nothing has to be an all-or-nothing solution…there are always intermediate steps that can be course corrected as actual results come in.
Totally agree with the concept of absolutely necessary to explore all possible alternative methodologies and at ALL stages!
While I have come to respect epidemiology much more in the last forty years or so, especially after the very clear results of the asbestos findings in late 70 era, it is basically an aggregation of anecdotal reports, albeit now accepted as statistically valid within limits.
Actual hard data has got to be more solid, especially with the small numbers we are still dealing with for this virus; it certainly seems that we will need a sample of at least 1% before any predictions can be generally considered reliable.
And those predictions may be completely over ruled in days by the speed of mutability of the virus, as has been shown clearly by the results of the seasonal flu vaccines.
Another point that MCO brought up early on was the mass exit from northern Italy south when their spikes began, and that is likely to impact FL and other ”retreat” areas in USA similarly.
Already seeing news reports of Rhode Island and Long Island becoming overtly hostile towards “virus refugees” from NYC.
Even without snowbirds and refugees, Florida is going to be in dire straits since the governor is in denial and the spring break tourists have massively pollinated the virus all over the coastal communities and Orlando.
The problem is with the long latency and high level of asymptomatic spreaders, even entirely good-willed honorable people who travel will unknowingly spread the disease.
And the vacation communities do not have healthcare systems setup to support large numbers of sick people. Vacationers usually head home for medical care.
I would guess sanctuary cities or at least neighborhoods would have much lower infection. I think the areas most affected are wealthy areas that have people who travel. At least that’s what I see looking in Massachusetts.
‘Take oxygenation for example. It would seem to me there must be multiple drugs/therapies that increase blood oxygenation…delaying (or maybe even eliminating) the time-to-ventilator’
Sounds great!
There are NO SUCH things as of now. Those severely sick have virtually LOST their lungs to exchange oxygen. with ventilators support, their body has a CHANCE to repair it’s lungs while maintaining other vital organs!
Read how the corona ‘viciously’ attacks human body (especially lungs) at WSJ if you have access.
( MD – retired)
There are no drugs to enhance oxygen uptake?
I am not talking about prior standard of care…I am talking about alternative treatments that could be attempted to delay time-to-ventilator in the current emergency circumstance.
@timbers – the seeds were sown in the wealthy traveling neighborhoods, because they were the people picking it up.
But the bitter harvest will be reaped in the poor communities, where population density is highest, self-isolation is financially impossible, and medical care is not routine.
I’m concerned whether the right standards are being applied to the question of whether repurposed drugs are worth trying. Have they been proven through randomized, double blind, controlled studies? Seems too rigorous in the context of the urgency of the problem. Why not Is the chance of benefit greater than the risk of harm? And who gets to decide? Seems to me the patient and doctor are in the best position to make that determination based on the particulars of the case.
The notion that central planners should make one-size-fits-all decisions should be up for discussion just as well whether it’s about the level of interest rates or treatment of disease.
What you are saying about mechanical ventilation is not correct. Many people can survive mechanical ventilation with ARDS. Part of the reason the death rate is Italy has been so high is that they don’t have the ability to provide ventilation to everyone who needs it.
Timbers
The early phase was the “travelers”, but it’s moving now more toward high density cities that don’t follow isolation well, with NYC being the most dense by far, and New Orleans failing on Mardi Gras. I don’t think immigrants are an issue in isolation.
This will be really tough on NYC, which is the most dense population area in the US by far.
Happy1 – “What you are saying about mechanical ventilation is not correct.”
Robert (below) cited a report from an ER physician who said:
“Worldwide 86% of covid 19 patients that go on a vent die. Seattle reporting 70%.”
I wasn’t saying vents are useless. What I was trying to say is that vents shouldn’t be viewed as the “be-all-end-all”, you know, if we can just get 100,000 vents, all will be fine type of thing.
More time and emphasis needs to be put not on vents, but on preventing people from ever needing them in the first place. If you get to the point of needing a vent, your chances of survival are just not that good.
Backwards,
You are correct. Way better to prevent than rely on mechanical ventilation. Just saying that death rate without ventilation if you need it is pretty much 100%. So even if 30% survive that makes a huge difference in a large population.
This will allow both GM & Ford to ramp up face mask production shortly.
Well, that’s certainly good news.
The White House had been preparing to reveal on Wednesday a joint venture between General Motors and Ventec Life Systems that would allow for the production of as many as 80,000 desperately needed ventilators to respond to an escalating pandemic when word suddenly came down that the announcement was off.
The decision to cancel the announcement, government officials say, came after the Federal Emergency Management Agency said it needed more time to assess whether the estimated cost was prohibitive. That price tag was more than $1 billion
Do you think a billion or more is a prohibitive cost? Compared to the ten or twenty trillion Wall St. is expected to ultimately get in bailouts that kind of money seems like chump change.
Unamused – what’s your expertise re ventilators? Are you an expert? Have you studied their use?
Because others I have read say differently than you. They have cited China’s experience with using them. Very, very, very few people were saved by vents.
These are hard decisions. Of course $1 billion would be worth it IF it actually worked, but just to throw out a billion dollars is stupid. I thank God some people are actually thinking this through.
Because others I have read say differently than you.
Couldn’t be differently from me because I haven’t expressed an opinion on the effectiveness of ventilators.
They have cited China’s experience with using them.
Who is ‘they’? And why are they so trusting of totalitarian Red China?
Very, very, very few people were saved by vents.
Why is that? Did they have a shortage?
Love the handle, by the way. It’s so you.
Unamused – maybe I’m reading you the wrong way, but I don’t think so.
I think the “Expert in Chief”, as you described him, is trying his best in a very difficult situation. One expert says one thing, and someone else says something different, and then there’s all the armchair experts who want to second guess everything you do, often because they want to see you fail.
Just because the governor of NY says he wants 40,000 vents doesn’t mean he’s right.
Links aren’t exactly allowed on this site, which is a shame. But I think if you did just a little bit of research on your own, edumacated yourself, you might actually learn something.
Backwordsevolution, if you’re worried abt $1 billion, you must bouncing off the walls the cielings and doors on reports the Fed plans to double yes double QE from 5 trillion (that’s 5,000 x 1 billion) to 10 trillion (that’s 10,000 x 1 billion).
Timbers – I wasn’t worried about the $1 billion. IF IT WOULD ACTUALLY WORK, it would be a small price to pay to save lives. But vents are not very effective.
I hadn’t heard about them wanting to double QE to $10 trillion. I was livid when the first QE was done.
“Never let a good crisis go to waste.” A backdoor bail-out of all the people who were about to go over a cliff.
Backwordsevolution, your response is puzzling. Because you spend much effort on a mere $1 billion for ventilators yet comparably so very much less on the $1.5 Trillions yes trillions with a T. Why the obsession with so small amount?
Timbers – vents and bailout money are two different topics. I was discussing the efficacy of vents.
It’s not the $1 billion for the vents that’s stupid. Gee, maybe we could throw $1.5 trillion at vents, but you’d still have the same outcome – it wouldn’t work.
Maybe I just don’t like “stupid”. People are losing their lives. There’s no time for stupid.
The call-off seems to have more to do with the shortly-thereafter invoked Defense Production Act than the $1 billion.
It sounds like Trump gave GM a couple days to be patriotic and noble but GM insisted on $1 billion before 1 ventilator got assembled…and having the option, Trump went with the DPA.
My question is whether or not GM/Ford are really the best mass producers (assemblers really) to place too much exclusive faith in – their performance over recent decades is not stellar…otherwise they would be Toyota.
Weeks could pass before the PowerPoint presentations are done…let alone ventilator 1.
Hopefully, the US still has other mass assemblers domestically located (PC makers? Printer makers? Appliance manufacturers? Etc….candidates requested btw) capable of integrating the 700 or so parts apparently required for a state of the art ventilator. Hopefully they are also in discussions.
(And how about the 700 suppliers of those parts…)
Or, hopefully there are enough lower tech machine shops capable of putting together the lower tech, lower resource DIY ventilators the MIT and Rice engineering teams have apparently prototyped. And hopefully more will kludge together.
Failing both (which I think is possible), and assuming things get worse, the best hope for lowering simultaneous ventilator demand may lie in slowing the medical progression to ventilator via alternative intermediate stage treatment modalities (or at least testing them starting now).
The consensus trmt is the consensus for a reason, but it is also yielding unacceptably fast progressions to ventilator. As we get closer to a crisis point on the ventilator end (if we do), then we are going to be compelled into triage decisions anyway.
Perhaps less profound ones can be made at earlier stages of trmt and I hope research is proceeding in this area.
But the public talk is almost all only about ventilators and front end vaccines (which are way off…in contrast to the dozens of less publicized existent drug candidates that translational med experts have already identified)
It might not be a bad time to reflect on an example of a geometric progression: the legend of the reward offered to the inventor of the game of chess in India a thousand years ago. The inventor was a mathematician and asked the ruling mogul for one grain of rice for the first square, two for the next, then four, etc, until all 64 squares were covered. The mogul was rich and thought a few sacks of rice, or a few hundred was no big deal.
As it turns out by the 40 th square it takes a billion grains and to cover the last one, 18 followed by 18 zeros, or enough to cover India with a carpet of rice several feet thick.
When a biological infection of anything starts the initial small numbers don’t matter as much as the progression. So while we talk of ‘epidemics’ of obesity, diabetes, car accidents etc. because there are more every year, they aren’t literal epidemics because they are increasing arithmetically not geometrically. For obesity to be a literal epidemic you would have to be able to quickly catch it from someone else and then infect someone else.
In the chess board example the rate of ‘infection’ is low. Each grain of rice only ‘creates’ two on the next square. If each grain created four (as in one carrier infecting 4) the progression goes: 1, 5, 25, 125, ….
Which might cause even a mogul to think that this reward could get expensive.
Nick,
But an underappreciated corollary would seem to be that anything that delays the interval between geometric steps or alters the exponent of growth, can have profound implications as to the timing/scale of endpt results. It is inherent in the process itself.
That is the essential logic of distancing/self isolating…to delay the progression and/or alter the exponent of growth.
But I don’t think that has been communicated well by the pols.
If they said something like “each day of additional lockdown is expected to lower simultaneous ventilator need by x” would go a long, long way to getting more people on board, for longer.
Voluntarily.
Well said. Now we need Fauci and Co to get De Blasio, Cuomo and Trump to just agree on a few numbers and roll with a common messaging…
Good point. There is no time function in the simple math geometric progression as there is real life. No doubt the sophisticated models can build that in.
The speed of some blights (plant epidemics) is also remarkable. The blight that struck the Irish mono-culture potato in the 1840 ‘s hit all at once. There are a few microbes greatly feared by brewers of beer and wine. One You-brew employee told me that when it hits they throw out everything and then boil all equipment for ten minutes. The most vulnerable point is just before fermentation begins because alcohol is a powerful deterrent to most ‘bad’ microbes.
Good news from BC.
Modeling has indicated that we are now on a trend that is close to what S Korea experienced. S distancing and testing has been pretty robust. Only real problems are some young people incidents and a few restaurants defying closure orders in Vancouver. However, they were shut down and fined. Our mortality rate seems higher than it really is due to a couple of Vancouver area care homes that became infected at the start of the outbreak. If you look at the population as a whole it is quite low, and overall, still below the rest of Canada even though we were the first to experience cases. The Province has now outlawed any care workers traveling to other work sites, and plans to put this directive into law when the crisis is over. For now, it stands by order from the Provincial Health Officer.
A casualty has been other hospital patients and their families. My father-in-law is in final days at a local regional hospital. We can’t visit, at all. (failing heart valve that cannot be replaced due to his age and asthma). However, we are now able to bring in his shaver and a cell phone as his Ipad gave up the ghost. The head nurse will meet my sister-in-law at the front entrance and take them up to his room…..AFTER she has them sterilized. Throughout the Province they have emptied hospitals as much as possible, have refurbished critical care equipment + ventilators, and more is coming from the Feds. We have enough ICU beds to meet the Italy scenario, and plans are underway to re-purpose public facilities for a ‘just in case’ more beds are needed for non Covid 19 patients.
As the health minister said, “We are hoping the S Korea level holds, but still preparing for worst case scenario. ”
“Dix said there are now 4,295 vacant hospital beds across the province as health authorities prepare for more cases.
Seventeen people have now died of coronavirus in B.C. The majority of the deaths in B.C. so far have been linked to North Vancouver’s Lynn Valley Care Centre.”
“On a positive note, Henry said 396 cases have now recovered, accounting for 45 per cent of the province’s total to date. Dix said 121 of those recoveries were confirmed in just the past 24 hours.
On Friday, Henry and Dix released new modelling data that shows B.C. may have avoided a “worst-case scenario,” with Henry expressing optimism that social distancing measures have begun to flatten the curve in the province.”
BC started to plan in January and the health officials are in charge of all policies. (Dr Bonnie Henry). She has the legislated authority to overrule all jurisdictions.
It will be interesting to see if later true randomized testing shows C19 infection/recovery to have been significantly more widespread than is currently believed. That would drop the mortality rate significantly.
As you point out, the overall mortality numbers so far are not huge and with a significant concentration in a few old age homes.
If true random samples come back with high infection rates, the understanding of C19 will likely change. There be more (and less) going on in the C19 process than we currently understand.
Paulo:
BC still has a fighting chance to bend the curve.
Not Ontario! Bragging about reaching 2,400 tests per day this week!
I see daily health updates from every province except Ontario! They seemed to have decentralized to regions!
The data on the US is getting better, Wisdom Seeker, and is now sufficient for preliminary statistical analysis, within certain limits.
There are large portions of the US population that are not under restriction, but should be, and others where restrictions are pointedly flouted and resented as political attacks on you know who. Therefore the data can be expected to improve exponentially for some time. Present projections are for the official mortality count to reach six figures in a few weeks, depending on how well the disinformation campaigns go and how long it takes to ramp up the repression of information.
Not sure I approve of your misanthropic sense of “getting better” and “improve”. A grim picture. Francesco’s summary of unofficial mortality levels indicates I must scale my estimates upward from the official counts far more than I expected.
Care to take a guess at overall US population a year from now? Will we need to repeat the Census?
IMO, Una was referring to the Quality of the data, not the actual numbers of cases, etc.
However, having said that , I disagree with the ability to derive statistically reliable information on which to predict future events from the small sample of population data so far. Perhaps I am being overly cautious, but it seems politicians are ready able and willing to base policy decisions on ANY good news, no matter how sketchy the data that news is based on.
STAY HOME folks,,, currently the only way!!
Thank you.
Your overly political take on things is tiresome.
Right now, metro NYC accounts for almost half of all confirmed cases in the US. Is this a hot bed of POTUS support? Do NYC residents see COVID related warnings as an attack on POTUS? Come on.
It was initially about places where people travel from Asia and Europe. Now, it’s about population density and how well people socially isolate. The people ignoring social isolation are young people and mostly urban (NYC, New Orleans, spring breakers in FL). NYC is orders of magnitude more dense than any other US city, of course it’s going to be a hotbed. The virus isn’t exactly tearing up flyover country, it’s just not as dense as either coast. POTUS isn’t helping but it’s more about how people live than about a politician you don’t like.
Right now, metro NYC accounts for almost half of all confirmed cases in the US. Is this a hot bed of POTUS support?
Probably not. But it does explain why the request for 40,000 ventilators was rejected.
The problem I see is that S Korea, probably the best case scenario for managing and suppressing this pandemic, and the most transparent, is STILL discovering new cases of COVID-19. About 100 reported today.
So this absolute BEST CASE SCENARIO country, which the US is about two orders of magnitude different from in terms of the social discipline needed to keep this pandemic from continuing to explode, has managed to Bend The Curve, but it still ain’t going down to zero. I’m guessing it won’t go down to zero for quite a while.
More trillions from the Fed and Congress!
I just wish all this should end lord please heal the world
It used to be “Praise the Lord and pass the ammunition”.
Now it’s “Praise the Lord and make the facemarks”.
Better yet: “Praise the Lord and wear a facemask.”
When this global catastrophe is over, probably by May, three things need to be done.
1. China must clean up. Stop the wet markets. Stop the wild food. Clorox everything. Join the modern world.
2. The West must revisit its antivirus plans. They have been a disaster. Totally unprepared. Nobody learnt from SARS.
3. The West must stockpile 10 billion surgical masks.
4. The West must wear masks and gloves in public, like the daily commute. Copy Japan. Change the culture. There must be no second wave in 2021.
5. There will be 1-2 decades of “austerity” to pay for it all. Government largesse will reduce. Everyone will tighten belts. It will be well into the 2030s before the West recovers.
Five things :-)
Given the branching of the virus and the possibility that it will evade vaccines like flu does, we might need local production capacity to make daily (disposable) or monthly (reusable) face masks for everyone on the planet for the next couple of years. Just to deal with this pandemic. And then maintain that capacity for the next pandemic wave.
The culture change needed for Point 4 is already swinging, you can feel it in the air. The fact that Science magazine (flagship for science in the US) raised the issue is a big step forward.
When this global catastrophe is over, probably by May, three things need to be done.
May of what year?
R2D2.
You should google the rates of rise of COVID-19 in your area to make a more informed assessment
In my area, things are still quite, but the numbers have been doubling every 4-5 days for the last 3 weeks from the initial few cases, a classic exponential rise. Which means by May, we will just be hitting the deluge.
It won’t be over by May 2020 for sure. It may not be over by May 2021 even
1. Wet markets are not the problem. Often the type of animals are the issue. Lets say India also has wet markets even as of now. The meats are mostly traditional (chicken+pork+beef) and sea foods (fish+others). Bat soup and pangolin meat must be banned.
2. Healthcare for all must be the first and foremost priority regardless of cost and economics.
3. Once if everything is over, it will be open borders vs. abortion.
Thought you were Michael Engle for a minute…
Your optimism is misplaced.
1. This is not a uniquely Chinese problem. The real issue is the overuse of antibiotics in the production of meat in the largest Eastern countries. It’s a perfect incubator for drug-resistant disease strains.
2. What anti-virus plans? We had plans. You know who tore them up and disbanded our epidemic response department.
3. The West will stockpile nothing, because ‘just in time’ delivery as a model is too profitable to just replace. Warehouse districts will not revive unless a massive spending initiative is passed, which will not happen because it doesn’t serve the profit margins of the private sector.
4. Not going to happen either. Not unless the death toll is suitably high. American exceptionalism weathers all ills.
5. The West will never recover. The power-paradigm has shifted. There is no East or West in this new world, only Top and Bottom. Unless you make more than a million dollars annually, you are part of the bottom. It’s your new job to fight among yourselves for the table scraps, and suck up to the Top, and by god you’ll like it or you’ll be un-personed.
Frankly I’m shocked that with so many comments on here, not one mentions the positive news coming from abroad and domestically. That being success with a combination hydroxycholoroquine and Zythromyxine treatment.
There are studies already out showing its efficacy from multiple countries.
Many Nations have ALREADY been using it, issuing official govt guidance for treatment for Covid.
Some doctors are prescribing it domestically off label and there is anecdotal evidence showing full recovery!
It’s cheap, proven for other ailments, easily produced, known side effects, etc…..
NY is conducting a trial with many patients.
WHO is finally conducting it’s own multi nation trial.
This is really huge news and very positive!
Don’t take my word for it, just Google it and get past the political bias BS and read about it!
That being success with a combination hydroxycholoroquine and Zythromyxine treatment.
You must mean Azithromycin. There’s no such thing as ‘Zythromyxine’.
The research paper cited (Gautret P., et al) has already been discredited and verges on scientific misconduct. It’s a very poor paper with plenty of conflicts of interests.
Lots of disinformation out there. For example, Stanford Health Care posted an “IMPORTANT NOTICE” on its Web site: “A widely circulating Google document claiming to have identified a potential treatment for COVID-19 in consultation with Stanford’s School of Medicine is not legitimate.”
Leave science to the scientists. Politicians can be expected to do it badly, especially those who are notorious for rejecting science when it contradicts their messaging.
Not as unquestionably great as BD makes it sound like.
Not as unquestionably dubious as Una makes it sound like.
Been in testing in NY since Tuesday, so maybe some preliminary feedback domestic-sourced soon.
The fact that some states moved to clamp down hard on CQ/HCQ scrips is *maybe* some limited evidence of insider Pol knowledge tending to the positive side…they don’t want general runs on a near term finite supply.
I don’t think high-screech statewide bans were put in place because of one “self help” aquarium product poisoning.
I didn’t say it was unquestioned, I said there is a ton of positive signs coming from many different sources that should absolutely be considered.
Which scientists should we leave science to? The ones who work for the pharmaceutical industry?
You worry too much Mr. Backwards. I think we can find you some who will toe the Party line.
You are correct, I am not a scientist it epidemiologist or virologist.
I am simply going by the small studies I have read, watching the actions of other govts, listening to multiple first hand accounts by both doctors and patients.
Based on all the above and some common sense, I think there is a lot to be excited about for treatment.
Broker Dan – I agree with you. I think these two drugs, in combination, are most promising. It could be they need to be administered early. Once the lungs are in a cytokine storm, where your immune system is going full throttle (what happened I believed with the Spanish flu), it might be too late.
“A cytokine storm is an overproduction of immune cells and their activating compounds (cytokines), which, in a flu infection, is often associated with a surge of activated immune cells into the lungs. The resulting lung inflammation and fluid buildup can lead to respiratory distress and can be contaminated by a secondary bacterial pneumonia — often enhancing the mortality in patients.”
In the end, it can be your own immune system that ends up killing you.
Stay healthy.
Yes, you should discount everything I wrote because I misspelled the antibiotic whilst typing on my phone.
Sheesh
Can you comment on the 2nd study just published 2 days ago, of 80 patients?
Admittedly, I know nothing about this French doctor, however, he isn’t some no namer operating out of a hole in the wall office quack either.
Pretty impressive resume:
Didier Raoult (born March 13, 1952 in Dakar, Senegal)[1] is a French physician and microbiologist. He holds M.D. and Ph.D. degrees and specializes in infectious diseases. In 1984, Raoult created the Rickettsia Unit at Aix-Marseille University (AMU). He also teaches infectious diseases in the Faculty of Medicine of Aix-Marseille University, and since 1982 has supervised many M.D. and Ph.D. degrees.[2]
Since 2008, Raoult has been the director of the Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes (URMITE; in English, Research Unit in Infectious and Tropical Emergent Diseases), collaborating with CNRS (National Center for the Scientific Research), IRD (Research for the Development Institute), INSERM (National Institute of Health and Medical Research) and the Aix Marseille University, in Marseille. His laboratory employs more than 200 people, including 86 researchers who publish between 250 and 350 papers per year and have produced more than 50 patents.[3]Raoult has also been involved in the creation of eight startups.[4]
BD,
I can’t comment on the quality of any one individual study, but I will make a general observation based on a fairly decent amount of time spent on Pubmed (US gvt’s well linked database of medical research papers from around the world…over 30 million of them, on every health topic, going back in some depth to 1965)
Even with a primarily successful treatment, early on you are going to see a lot of small studies, with at least some mixed results…since the sample sizes are so tiny, the studies done so fast, or the patient populations incompletely understood/semi-standardized.
There are unlikely to be definitive conclusions early on…but given the potential size of the problem, and the severity of bad outcomes, I think/hope the “standard of proof” will be somewhat loosened.
This is especially true since the adverse effects testing of CQ/HCQ is long, long since past and mass real world utilization has been going on for decades. The risk-benefit of CQ/HCQ has been found acceptable for conditions less serious than C19.
The real question is efficacy and if any better alternatives are in the immediate offing…CQ/HCQ seem further down the road than almost anything else, even the dozens of repurposed drug candidates that translational med researchers have found computationally promising.
My guess is that many/most/all of those will be in efficacy testing shortly as well. They may have already started.
I read it and do see what you are referring to in the “combiination” comment.
It is interesting however, what other readers here think about this medical report referencing HCL as one of the anti-viral treatments.
Lots of “snake oil” comments on here, yet, you have posted a paper which identifies said drug as an anti-viral treatment for C19.
“that quinine only works on early patients, and can never be used on women who plan or are giving birth.”
Taking everything you said as true (but I’m not going to an unknown download file to confirm), that is still a sh*t ton of people that could be treated and another sh*t ton of further spread impeded.
And, as larger trials are in effect as we speak, we will have more info in the not distant future.
And, there is a substantial line of plausible drug treatments (many of which have already been through adverse effects testing) waiting in line behind CQ/HCQ, waiting (or already undergoing) efficacy trials.
Cas,
Curious what you base this comment on:
“CQ/HCQ seem further down the road than almost anything else, even the dozens of repurposed drug candidates that translational med researchers have found computationally promising.”
Why further down the road? Which repurposed candidates are you referring to? Are there studies showing their efficacy in treating C19?
I’m genuinely curious.
BrokerDan,
First, translational medicine pipeline of existing drug candidates,
https://www.sciencealert.com/a-treatment-for-covid-19-might-already-exist-in-old-drugs-we-just-need-to-unlock-the-right-combination
My guess is that efficacy testing has probably started on a lot of these candidates.
As to CQ/HCQ being further down the road, I was simply referring to the small number of positive efficacy tests (China and France) using small sample sizes. CQ/HCQ had been attempted earlier to some degree of apparent success, so they were…further down the road.
But the other “translational” candidates will catch up in testing…their big advantage is that there are over 20k existing drugs that have apparently already gone through the time consuming adverse effects trials.
Now they only need efficacy trials.
The translational researchers use what is known about these drugs’ chemical pathways/mechanisms of effect to computationally match them to what is known about C19…and derive a subset of drug candidates with greater probability of impacting C19.
One study I read indicated it was no better than normal care including bed rest, hydration monitoring, etc.
Larger scale, more scientific studies are being done now.
You may satisfied with laying around drinking water and seeing what happens, but, I am not.
I’m trying to be proactive and monitor all new info as it becomes available.
If it came down to it, I’m taking whatever *might*work instead of what you recommend. This bug is deadly and the immune system needs help. Ain’t just the flu, bro
You’ll take what’s available to you, and if you get sick during a giant wave of cases, that might be tylenol and not much else. So stay home and try not to get sick. Maybe in 6 months the situation will look a little better and cure rates will improve. If you can make it 18 months maybe you can even get a vaccine.
Interesting article I just read in Bloomberg about David Ho, Time Magazine’s Man of the Year in 1996 for his discovery of the class of protease inhibitors which were the first drugs able to successfully treat AIDS. The field of viral treatment has advanced significantly since.
Great article with lots of science based approaches to attacking this and future coronaviruses
Chloroquine and azithromycin? Haha. Not. Might as well try Laetrile or Jimmy Bakker’s Silver Solution
Lots of smart people working on this, something will be found that works, but not in a few months
Broker Dan,
I generally don’t allow comments that flog meds, supplements, miracle cures, etc. because some readers might actually take them seriously.
Thanks for saying this Wolf, its true, everytime there is a pandemic in USA history, 1,000’s of snake-oil salesman show up all over the country with their miracle cure.
Why not read a report from those in the trenches about what is actually working, and not working.
In fact most of these ‘internet cures’ have all been tried and tested on live patients, but still only a very few drugs actually relieve the patients.
Understood. Let me say this then.
There is a large trial happening right now in NY, started last Tuesday.
Let’s re-visit this conversation in another week once we can see the results. I’m hopeful, that’s all.
No, Dan, we won’t “revisit.” We don’t promote meds, supplements, and miracle cures here. Not happening. It’s not up to me to decide what works and what doesn’t. I delete just about all of them.
There are lot of really smart people working on treatments, cures, vaccines, and the like. And some of the them are going to be safe and effective, and others won’t be. And it’s up to the researchers, the regulators, and the healthcare providers to decide, not me or you.
BTW,
No, I’m not a healthcare professional.
No, I don’t own any stock in anything.
No, I’m not offering any medical advice whatsoever.
Not selling anything.
I’m a Real Estate guy.
I’m simply following C19 like the rest of us and reading public info.
Nice write up.
One point that I’m curious about but have not heard a word on as yet.
The early part of dealing with this is to identify and “isolate” the infected, for which testing is ideal. It certainly seems like testing is ramping up in the US, between Cepheid, Thermo, and now Abbott, it seems likes it’s moving forward. The advantage is that the technology for this was always in place. The trick was to get the right reagents for the testing, once they have that, it’s a matter of sticking it into a thermcycler.
The latter stages where the critically ill are also receiving a lot of attention. Ventilators to help stabilize those who are fighting for their lives. Newsom had a press conference at Bloom Energy today talking about how they were refurbishing ventilators. Oddly enough, Bloom is pretty much right next door to Cepheid, so double bang for the PR buck. I am impressed by the job Newsom is doing here.
But the one area that is missing is what happens to the pack in the middle, where people are infected and becoming symptomatic, but not critical to the point of needing a ventilator. Not much talk going on so far about treatments to keep those people from becoming critical cases, I think there are nearly a dozen drugs out there now (usually some type of anti-viral) that is supposed to help alleviate the symptoms and slow the infection. But in the US, there isn’t much talk about that yet. I don’t think vaccine will play into this until much later, probably in 2021 if they manage to develop one, this will get into the annual flu vaccination cycle.
MCH,
Agreed, other than the ventilator issue (which is an endpt in medical progression/treatment) there has been very little discussion of intermediate medical treatment issues.
There has been marginally more coverage on front end issues (Chloroquine wars) but really very little discussion of other possible trmts.
Perhaps that is to absolutely maximize lockdown compliance, but considering the endless hrs of political hash and rehash on cable…perhaps some more practical medical coverage could be fit in.
I am so weary of idiotic media coverage on the subject. It is all about sensationalism.
Chloroquine is a prime example, just because an idiot said something about it, and got broadcasted all over, people are looking to it like some miracle cure, never mind that there are no specific trials associated with this, and worse, the information given was incomplete and inaccurate. The media “debunked” it, but there was kernels of truths to the situation, so instead of reporting the situations accurately, it became a story about the orange haired one spreading misinformation.
Then there is just an appalling lateness in coverage on certain items. Back in early February, I read in non-Western media about China using CT scan as a back up to identify COVID-19 infection due to certain build ups that were seen in the lungs, and around a week or so later, there were several reports about blood transfusions from previously infected patients to those critically ill that was showing efficacy.
I literally fell out of my chair laughing about two or three weeks ago when CNN or some other western news outlet started talking about CT scans as verification and called it breaking news, and then seeing the blood transfusion thing this week. I wonder whatever happened to the days of honest journalism… everything now is geared like a frigging reality TV show.
MCH,
There are studies and trials that have happened and are ongoing.
Not sure why you discount it immediately. The same media you “laugh at” is the same media that debunked it?
@Broker Dan
I am not discounting things. My point is that the media is in general so interested in discrediting Trump that they don’t consider the nuance of the story, the headline is always Why Trump is bad. There isn’t that much talk about ongoing trials except that as a mention off to the side. The nuance isn’t given the same headline as the lie. I think that part tends to be important. Consider how much air time is given to trials.
In terms of real journalism, I see more reality TV than I do credible stories. In times like this, when there is credible information, for example the CT scans as an alternative diagnostic to supplement the RT-PCR testing, it isn’t put up until much later. Then only as a side note. This was happening in China in early to mid February. The first time it made it into the headlines for CNN was I think about tow weeks ago. It feels like half of these journalists are waiting for things to be outsourced to them.
The adage “if it bleeds, it leads” seem to be never more true. Especially in the click bait era of journalism.
MCH,
I can agree with that.
@Broker Dan
Also note that today, FDA provided emergency authorization for Chloroquine, and guess what actually happens to that relevant piece of information.
Nowhere to be found on the front page of CNN, buried in the unseen sections of ABCnews site, and obliquely mentioned on Fox about four lines down (for the purpose of pumping up Trump).
Oddly, medically relevant and useful information to real people is ignored or buried in order to gin up head lines on all this irrelevant political fights associated with Trump.
Whatever happened to useful information like types of testing involved for COVID-19, their relevant accuracy, etc, the differences for example between the Roche and the Cepheid tests. Under what circumstances are Chloroquine or Remdesivir
Not a word. Why? The journalists of today have no background or training typically for this, it’s easy to write or say “everything should be science driven” without understanding any of the science. All great and attention grabbing headlines that means absolutely nothing. It’s just another way of trying to dumb down everyone.
And journalists wonder why there is such a mistrust of the news media in general these days. I get more relevant information off of reading the comments here than at CNN.
From a population-level perspective, the best “treatment” for anyone with any symptoms is immediate isolation so that they cannot infect others (any more).
For the individual, best “treatment” is more rapid and accurate tests, so the doctor knows what they’re dealing with and can provide whatever intermediate-stage therapy helps most. Can’t get to the COVID-treatment stage without knowing it’s COVID. In a few weeks I suppose that won’t matter b/c pretty much everything will be COVID.
The New Orleans doc quoted elsewhere on the thread says a prone (stomach-side-down) position helps with oxygen supply.
I’ve seen various reports saying NOT to take ibuprofen or apply steroids, as these are counterproductive. (Note: also true of high-dose aspirin during the 1919 pandemic flu.)
There are thousands of drug trials underway and hopefully some of them will turn out well. They aren’t getting the news yet maybe b/c there isn’t enough positive data?
Hopefully CDC will update its clinical guidance soon, the current version is from March 7 and the world has learned a lot in the past 3 weeks.
Data will be useful up to a point in saying how many are infected, but without accurate knowledge by the masses, containing the infected will be challenging unless extreme measures are taken.
You can imagine a system where there is an app set up that indicates the immediate surroundings where an infected or a potentially infected person might be, it will allow the uninfected to exercise meaningful Social distancing. But the two problems with this in the West will be both a gross invasion of privacy (anonimization will only go so far) and a lack of ability. China is likely the only country where this might be possible, although it is technologically still not quite there since I don’t think they can fuse medical data with mass surveillance and AI to such a degree yet. On the technological scale, this is not possible in the west at all.
So, detection is useful but only to the extent the the infected knows they are infected and will be willing to act to the benefit of their fellow humans and not be a Covidiot or a Covdouchebag.
That why I think the middle stage is so important, right now, there is no good advice on treating mild symptoms or to prevent those with early symptoms from becoming worse.
In reality, the bottleneck (if this pandemic accelerates) will not be in ventilators, but having enough human staff to support the large swath of critically ill and the infrastructure around this. There is not enough infrastructure in the world to cover this if the situation really explodes, it hasn’t really done that yet.
Hence the lack of meaningful treatment to mitigate and slow the progression Covid-19 is I think a big blind spot for the world.
Put it another way, if you think about Covid-19 as a cancer, there is no equivalent of chemo, radiation, or anything else to slow or retard it’s progression, only detection and late stage management when the symptoms have worsened to the point where the patient is no longer able to support themselves. Except the differences are that Covid-19 acts a lot faster than most cancers, is infectious, and is forcing a slow collapse of infrastructure.
Speaking of blind spots, just read another article in Asia that they think a good part of the transmission is through children whose immune systems are stronger and can delay or fight off Covid-19 but remains sufficiently infectious to transmit the problem to adults who are less capable. I wonder when our media will pick up that nugget and call it breaking news.
Ignore the, you do not need to wear a mask. Wear a mask if you have one and gloves. My bro PhD in microbiology and experienced with viruses in SF, says wear a mask! Wear gloves ! I lucked out I have a n99 with a filter. I bought it last year for pollution on my trip to China. Never needed it. Who knew….
Bet:
Wearing a mask and gloves may or may not do a great job of protecting you. I can’t hurt.
But I think if an infected person wore a mask and gloves it would go a long way towards reducing the chances of spreading the virus to other people.
And county reports in the Bay Area are saying that during mitigation phase, everyone should act as if everyone else is infected.
So we should all mask up.
The greatest benefit to the general health of the population is delivered by drinking water that doesn’t kill you. Quite simple.
The greatest benefit during a pandemic is delivered by simple policy of the universal wearing of masks, (better hygiene, distancing, testing, isolation and quarantine when indicated).
Because once you get to hospital, you are a pretty hopeless case by and large.
But what do the politicians and state medical advisors tell us: masks are ‘useless and not needed’!
They are even trying that line on staff in hospitals, in Britain at least. It’s rather shocking.
My brother just wants us to be as safe as possible. If you are asymptomatic …
Makes sense to me that everyone should be wearing a mask. They do in the southeast Asian countries. They seem to have their stuff together a bit more than we do. I had asthma as a kid. I know already what it’s like to suffocate and gasp like a beached fish
Would not wish it on anyone . My lungs are great now,but I am not real keen to have them tested with this
This from an E.R. doctor in the front line trenches in Louisiana (highly technical, but note, especially for those advocating massive industrial diversion to crank out ventilators his observation that 80% of those going on ventilators die):
“I am an ER MD in New Orleans. Class of 98. Every one of my colleagues have now seen several hundred Covid 19 patients and this is what I think I know.
Clinical course is predictable.
2-11 days after exposure (day 5 on average) flu like symptoms start. Common are fever, headache, dry cough, myalgias(back pain), nausea without vomiting, abdominal discomfort with some diarrhea, loss of smell, anorexia, fatigue.
Day 5 of symptoms- increased SOB, and bilateral viral pneumonia from direct viral damage to lung parenchyma.
Day 10- Cytokine storm leading to acute ARDS and multiorgan failure. You can literally watch it happen in a matter of hours.
81% mild symptoms, 14% severe symptoms requiring hospitalization, 5% critical.
Patient presentation is varied. Patients are coming in hypoxic (even 75%) without dyspnea. I have seen Covid patients present with encephalopathy, renal failure from dehydration, DKA. I have seen the bilateral interstitial pneumonia on the xray of the asymptomatic shoulder dislocation or on the CT’s of the (respiratory) asymptomatic polytrauma patient. Essentially if they are in my ER, they have it. Seen three positive flu swabs in 2 weeks and all three had Covid 19 as well. Somehow this ***** has told all other disease processes to get out of town.
China reported 15% cardiac involvement. I have seen covid 19 patients present with myocarditis, pericarditis, new onset CHF and new onset atrial fibrillation. I still order a troponin, but no cardiologist will treat no matter what the number in a suspected Covid 19 patient. Even our non covid 19 STEMIs at all of our facilities are getting TPA in the ED and rescue PCI at 60 minutes only if TPA fails.
Diagnostic
CXR- bilateral interstitial pneumonia (anecdotally starts most often in the RLL so bilateral on CXR is not required). The hypoxia does not correlate with the CXR findings. Their lungs do not sound bad. Keep your stethoscope in your pocket and evaluate with your eyes and pulse ox.
Labs- WBC low, Lymphocytes low, platelets lower then their normal, Procalcitonin normal in 95%
CRP and Ferritin elevated most often. CPK, D-Dimer, LDH, Alk Phos/AST/ALT commonly elevated.
Notice D-Dimer- I would be very careful about CT PE these patients for their hypoxia. The patients receiving IV contrast are going into renal failure and on the vent sooner.
Basically, if you have a bilateral pneumonia with normal to low WBC, lymphopenia, normal procalcitonin, elevated CRP and ferritin- you have covid-19 and do not need a nasal swab to tell you that.
A ratio of absolute neutrophil count to absolute lymphocyte count greater than 3.5 may be the highest predictor of poor outcome. the UK is automatically intubating these patients for expected outcomes regardless of their clinical presentation.
An elevated Interleukin-6 (IL6) is an indicator of their cytokine storm. If this is elevated watch these patients closely with both eyes.
Other factors that appear to be predictive of poor outcomes are thrombocytopenia and LFTs 5x upper limit of normal.
Disposition
I had never discharged multifocal pneumonia before. Now I personally do it 12-15 times a shift. 2 weeks ago we were admitting anyone who needed supplemental oxygen. Now we are discharging with oxygen if the patient is comfortable and oxygenating above 92% on nasal cannula. We have contracted with a company that sends a paramedic to their home twice daily to check on them and record a pulse ox. We know many of these patients will bounce back but if it saves a bed for a day we have accomplished something. Obviously we are fearful some won’t make it back.
We are a small community hospital. Our 22 bed ICU and now a 4 bed Endoscopy suite are all Covid 19. All of these patients are intubated except one. 75% of our floor beds have been cohorted into covid 19 wards and are full. We are averaging 4 rescue intubations a day on the floor. We now have 9 vented patients in our ER transferred down from the floor after intubation.
Luckily we are part of a larger hospital group. Our main teaching hospital repurposed space to open 50 new Covid 19 ICU beds this past Sunday so these numbers are with significant decompression. Today those 50 beds are full. They are opening 30 more by Friday. But even with the “lockdown”, our AI models are expecting a 200-400% increase in covid 19 patients by 4/4/2020.
Treatment
Supportive
worldwide 86% of covid 19 patients that go on a vent die. Seattle reporting 70%. Our hospital has had 5 deaths and one patient who was extubated. Extubation happens on day 10 per the Chinese and day 11 per Seattle.
Plaquenil which has weak ACE2 blockade doesn’t appear to be a savior of any kind in our patient population. Theoretically, it may have some prophylactic properties but so far it is difficult to see the benefit to our hospitalized patients, but we are using it and the studies will tell. With Plaquenil’s potential QT prolongation and liver toxic effects (both particularly problematic in covid 19 patients), I am not longer selectively prescribing this medication as I stated on a previous post.
We are also using Azithromycin, but are intermittently running out of IV.
Do not give these patient’s standard sepsis fluid resuscitation. Be very judicious with the fluids as it hastens their respiratory decompensation. Outside the DKA and renal failure dehydration, leave them dry.
Proning vented patients significantly helps oxygenation. Even self proning the ones on nasal cannula helps.
Vent settings- Usual ARDS stuff, low volume, permissive hypercapnia, etc. Except for Peep of 5 will not do. Start at 14 and you may go up to 25 if needed.
Do not use Bipap- it does not work well and is a significant exposure risk with high levels of aerosolized virus to you and your staff. Even after a cough or sneeze this virus can aerosolize up to 3 hours.
The same goes for nebulizer treatments. Use MDI. you can give 8-10 puffs at one time of an albuterol MDI. Use only if wheezing which isn’t often with covid 19. If you have to give a nebulizer must be in a negative pressure room; and if you can, instruct the patient on how to start it after you leave the room.
Do not use steroids, it makes this worse. Push out to your urgent cares to stop their usual practice of steroid shots for their URI/bronchitis.
We are currently out of Versed, Fentanyl, and intermittently Propofol. Get the dosing of Precedex and Nimbex back in your heads.
One of my colleagues who is a 31 yo old female who graduated residency last may with no health problems and normal BMI is out with the symptoms and an SaO2 of 92%. She will be the first of many.
I PPE best I have. I do wear a MaxAir PAPR the entire shift. I do not take it off to eat or drink during the shift. I undress in the garage and go straight to the shower. My wife and kids fled to her parents outside Hattiesburg. The stress and exposure at work coupled with the isolation at home is trying. But everyone is going through something right now. Everyone is scared; patients and employees. But we are the leaders of that emergency room. Be nice to your nurses and staff. Show by example how to tackle this crisis head on. Good luck to us all
Robert – that was fascinating. Thanks for posting that!
I salute all the people in the front lines who are staking their lives to save others!
Thank you for sharing. Wonderful person you are. Thank you for being you.
Thanks, this is the most comprehensive post I’ve seen in any forum and the level of detail is very appreciated by this medical professional. I’ve seen 20 cases and have a similar take, but this is much more informed than my more limited experience.
Re – Progression from C19 infection/pneumonia to full blown ARDS.
I also wonder about acid-base imbalance problems developing with people under C19 pneumonia stress/pre-ventilator oxygenation…disrupted breathing patterns/volumes can throw the body’s fundamental acid-base balance out of whack…to the extent that the imbalance can actually denature proteins in the human body.
How is the immune system going to react if a ton of denatured, foreign looking proteins pop up all over the body? You would think it might be the kind of thing that might derange an already stressed immune system…which sounds a bit like what happens in cytokine storm.
Unfortunately, the few hundred/thousand experts in the area have been working on ARDS for decades (PubMed lists about 12000 papers mentioning ARDS) and have not found many good treatments (thus the ventilators).
You would think the semi-simple stuff was examined closely and ruled out decades ago…but who knows. Sometimes the experts are biased toward complicated answers/solutions.
Considering that likely a billion people are now sequestered with little else but internet access, it might be productive *to put them to work* re-examining assumptions and those 12k papers.
There is really no reason why this MF’er can’t be crowdsourced…at least at the research, prepatient stage.
That billion may have a long time to learn a lot more about a relatively small subset of medicine.
Thanks for all that you are doing to help those in your community. Stay safe!
This is a true story… happening right now.
My daughter-in-law had tremendous pain in her uterus area. She and my son lives in Brooklyn. She works in a Brooklyn hospital. She was told to go out of state and look for an ER!!! So my son drove to Stamford, CT.
My wife called the doctor and she was being convinced not to go to the hospital! They did anyway, and are now in E.R. Meanwhile, my son was not allowed to stay in the ER. He was asked to leave and wait in the car.
They went home to get fast chargers and battery banks. I have special ones ready all the time since I was hospitalized a few months ago.
Now, unless she gets admitted after an ultrasound, they will come to our home and quarantine. All New Yorkers are required to quarantine for 14 days. So I got the spare bedrooms ready; chlorox wipes, masks, etc. We will take turns dining. Unbelievable!
If she might be infected and in your house, don’t you have to quarantine also ?
Yes. We are quarantined already becuase all 3 states NY NJ CT have stay at home rules. I don’t want to get sick.
She was just sent home now. Scheduled surgery maybe tomorrow. Ugh.
I forgot, my wife and son were asked to wait from noon to midnight outside the hospital. Only patents allowed in.
Vit C daily. Zinc lozenges. Cardomoms and turmeric in rice. Vit D3 to raise WBC. Be well. Fear lowers immunity. Each day in fav spot in nature deep breathe get in touch with peaceful inner space. No ibuprofen or ferritin or st johns wort. Eat nutritious raw.
Iamafan,
If they may be scheduling surgery, what is the preliminary diagnosis based on the ultrasound?
(This does bring up the segregated hospital issue raised in other countries…that is, should certain hospitals/facilities be C19 only so that other facilities can more smoothly carry on all other medical procedures.
Ditto for the C19 only hospitals as well…their operation can be optimized too.
I think a strong case can be made for that but such discussions in US have barely begun)
New York has way too many people and way too many people coming and going to New York. They need a rotal lockdown or the numbers will keep growing.
Raxadian:
NYC’s major is busy working on a plan to do just that!
NYS’s governor is busy working on a plan to do just that!
Get out of NYC while you still can. I am taking my son and DIL and their dog into our house in Connecticut. NYC is a hell hole now.
Paging Dr. Snake Plissken (best badass name of all time), will Dr. Snake Plissken please pick up the white courtesy phone…
Ironically, we were watching that awesome movie yesterday AM when we got a frantic call from our son. All hospitals in Brooklyn rejected their emergency. Wife was in horrible pain.
Just escape NYC and go somewhere with less people.
Wolf I had to add this from the posting earlier. The death rate from pneumonia in Italy normally is 3-5000 per week.
I call BS on that number.
Italy has 60 million people and a life expectancy in normal times of about 80 years. So 750,000 die in a given year. (In 2012, 613,520 actual deaths reported BTW.) No way that 5000/week (250,000K/year) are pneumonias.
Per Istat (national stats institute for Italy), top 3 leading causes of death were ischemic heart diseases (75,098 deaths), cerebrovascular diseases (61,255 deaths) and other heart diseases (48,384). These accounted for 30% of all deaths in 2012.
Lower respiratory diseases (which would include pneumonia) was only 20,000 for the year.
COVID has 10K in a month, not counting the ones that weren’t even tested.
Followup: No other cause of death in Italy does >10,000 month. COVID is the leading cause of death in Italy right now. It isn’t over and in fact might just be getting started.
WS,
“These accounted for 30% of all deaths in 2012.”
A lot depends on how narrowly the categories are defined, but the big three (heart disease, cancer, stroke) tend to make up a very large percentage of deaths, so just 30% for the three listed sounds low.
Not saying that 3 to 5k per *week* for old style flu/pneumonia is right…but maybe per month?
50k per annum out of 750k sounds plausible for old flu and would put C19 at 2 to 3 times worse than old style flu/pneumonia, which also sounds plausible.
My broader pt, Istat categories notwithstanding, is that officially reported causes of death may be subject to methodological issues.
If you go in to a hospital for a general surgery, but end up with a pneumonia/ARDS that kills you (not uncommon – surgery can trigger ARDS) the proximate cause of death is respiratory…but it might not be reported that way – the stats may focus on the surgical motivation.
Fair enough, but if 600-750K die per year from all causes, that’s only 12-15K/week from all causes. COVID in Italy just killed 5K i the past week all by itself. No other single cause of death comes close to that. And especially not influenza which isn’t in the top 3.
Pneumonia is not a disease. It’s a symptom ‘fluid on the lungs’. Same Latin root- word as ‘pneumatic’ tire. The tire is filled with air, a fluid.
Pneumonia can have a bacterial cause, a viral cause or a non-biological cause. A very hard to treat version of the latter can be caused by inhaling gasoline fumes while siphoning gas.
The proximate cause of death from the corona virus is pneumonia. But as a New Orleans respiratory therapist has told Propublica, he has never seen fluid build up so fast. The patients on ventilators have to be restrained when the mammalian drowning reflex kicks in. They struggle to remove the tube, even though it is their source of oxygen.
To be sure, ‘ordinary’ pneumonia is a typical way for the aged to die. But here we have pneumonia of non- ordinary type that kills non-aged patients at a far higher rate than ordinary.
NK,
What are the specific non-aged mortality rates for old style flu vs. the non aged mortality rates for C19?
“Much higher” can be measured along two different axes.
And isn’t pre/post-intubation sedation the standard?
And aren’t fluid drains surgically installed and/or many ventilators equipped to also provide drainage?
Coronavirus disease (COVID-19) advice for the public: When and how to use masks.
If you are healthy, you only need to wear a mask if you are taking care of a person with suspected 2019-nCoV infection.
Wear a mask if you are coughing or sneezing.
Masks are effective only when used in combination with frequent hand-cleaning with alcohol-based hand rub or soap and water.
If you wear a mask, then you must know how to use it and dispose of it properly.
Before putting on a mask, clean hands with alcohol-based hand rub or soap and water.
Cover mouth and nose with mask and make sure there are no gaps between your face and the mask.
Avoid touching the mask while using it; if you do, clean your hands with alcohol-based hand rub or soap and water.
Replace the mask with a new one as soon as it is damp and do not re-use single-use masks.
To remove the mask: remove it from behind (do not touch the front of mask); discard immediately in a closed bin; clean hands with alcohol-based hand rub or soap and water.
WHO World Health Organization
@Carlos: Thanks for that! The first two points in that WHO guidance were pre-pandemic and is out of date.
Everyone in an infected region under shelter-in-place must presume they are infected, and everyone else is infected, and act appropriately to avoid spreading the infection. Doesn’t matter if you feel healthy – 1/3-1/2 of cases are asymptomatic spreaders per Diamond Princess, Iceland and recently-leaked Chinese data.
So everyone should wear face covering whenever outside the home. It doesn’t have to be a surgical mask. All substantial face coverings reduce droplet spread and raise personal awareness to reduce hand-to-mouth spread from contaminated hands.
The rest of the guidance still applies.
Greetings From India Wisdom Seeker,
In India number of total cases (918) and deaths (19) seems to be contained till now (atleast as per official government statistics, unsure about how reliable this stats are). However the announcement of lockdown has the resulted in chaos in certain parts of country especially in delhi and Utter Pradesh. When lockdown was announced initial reaction of people was to rush immediately outside to buy groceries, medicine etc. When this buying spree was over, people belonging to rich and middle class (they have enough financial muscle to withstand a 21 day lockdown) are successfully locked up in their home. However migrant labourer (very large part of cities’ population) are rushing towards their home in rural villages in droves increasing risk of spread of virus resulting in overcrowding at train and bus station . See this Photo:-
https://mobile.twitter.com/NBTDilli/status/1243852275937759232
To prevent this goverment decided to stop government train and bus services and restricted interstate movement. Howver, many labourer decided to head home by foot essentially walking 300 to 400 km. See:-
https://mobile.twitter.com/gurdeepsappal/status/1243564721048961026
https://mobile.twitter.com/Geeta_Mohan/status/1243531869305495559
While some started to use private bus services which are operating even though goverment has ordered their closure too. These has resulted in chaos at the interstate borders where thousands are gathered in lines so they can enter their home state and then go to their home.
See this twitter video:-
https://mobile.twitter.com/LamaPrawesh/status/1243873440202809345
The primary reason that these people are heading home is that is these migrant workers are mostly daily labourer who are hired and paid on daily basis and thus they have become unemployed in lockdown with very little cash and will suffer from starvation if stayed in cities. Thus, state governments decided to try to provide food and shelter to them so they stop leaving, resulting in shortages of food due to large number of people.
https://mobile.twitter.com/AnjaliB_/status/1242777027763003393
These has happened for the whole week.
Cause of all this seems to be lack of proper planning and execution of lockdown by the government. I hope situation improves soon as at this rate lockdown will increase the spread of virus instead of containing it.
It is strange that since one of the major reasons for having a public health authority (and I am definitely including the US CDC and individual state authorities here) – if not *the* major reason for health authorities – is public epidemic control, then why so very, very few preplanned structures/standards appear to exist for varying degrees of lockdowns/quarantines for neighborhoods, metros, states, and regions.
Where have decades of budgets been allocated…if not to such preplanning?
There don’t seem to be many leaks that Trump is willy-nilly ignoring actual CDC plans (despite an ocean of other accusations) which suggests there never were many such plans.
WTF?
Isn’t that a core function of epidemic preparedness? In addition to medical treatment?
Desai, thank you for the update! Hopefully they issued the lockdown order early enough that the nation can work through the “changeover” issues before the pandemic really gets going. Food distribution is critical. I hope the educated and aware are able to swing public opinion quickly so everyone understands the importance of staying separated as much as possible and wearing face coverings.
Please keep us informed!
I am prepared to die if needed but I deny to live in fear but I am not reckless.
May be it’s nature’s way of purging things out from the face of the earth.
I’d much rather live in fear for a few months, than die needlessly. Just saying.
As a resident of MN, I can tell you that the testing here is not up to par. If you have so much as a sniffle or a cough you are told to stay home and do a virtual Dr. Visit. They aren’t testing people until you end up bad enough to go to the hospital. Therefore the numbers in MN are not accurate. The closures of places of gatherings last week and throughout the next 2 weeks will definitely help slow the spread for this first wave bit even our Governor admitted that when all is said and done, somewhere around 80% of us will have gotten infected. This battle is LONG from over.
Chloroquine has been used in China and S. Korea during the current epidemic. It is manufactured in India, China, Germany and elsewhere. India, Germany and France have banned the export of chloroquine.
Convalescent plasma treatment was used successfully with the Ebola epidemic and in Wuhan starting February. The FDA is allowing use of plasma from recovered coronavirus patients in sick patients.
From the first US COVID-19 case to over 100,000 cases in less than ten weeks.
If US hospital capacity is exhausted, the mortality rate will rise. Hospital staff have been quitting, out sick and dying. Severe cases can last 3-6 weeks.
I’m very hopeful that HCL + ZPak is the real deal.
Been reading/hearing encouraging things.
Where?
ED,
Just Google…there are plenty of positive and negative takes.
It’s absurd, you think Italy and Spain and NYC would be letting people die by the thousands if a great cure was floating around?
Probably.
If anyone still doubts where the priorities of our government, elected officials, the fed and anyone else in a position of power in this country lie, take a look at the below from the governor of NY.
Andrew Cuomo:
“New York is the financial sector. You geographically restrict a state, you would paralyze the financial sector,” Cuomo said. “You think the stock market has gone down — it would drop like a stone.”
Really? That’s your chief concern Mr. Governor? The stock market??? So WHAT if it drops like a stone? Would that be the end of the world? I guess it would….
He was talking in the context of Trump’s obsession with the stock market.
If trump is focused on propping up the stock market at all costs, aside from being illegal, trying to mandate an isolation of Manhattan would make it drop like a stone. Would be counter productive to what he wants to see anyway.
As horrific and frightening as the Covid-19 outbreak is, what is even more terrifying to me is the reality that all the deaths to date worldwide represent less than one day’s growth in India’s population in the past year. The same could be said for China’s, and any number of other countries around the globe. The natural world is under siege by the masses of humankind, and what we are experiencing presently is not an aberration. It is likely the new “norm”, and perhaps only the first round of population destruction to visit us. If this scourge attacks mostly older people, the absolute numbers of people may decrease briefly, but humankind’s ability to ” grow” population will be interrupted only briefly if at all. Also, while we are trying to figure this conundrum out, how many of the higher order species, mammals, fish and birds for example, will survive? Bacteria and viruses will always be with us, but will anything else survive? The thing of nightmares!
B
Focus on your sphere of inflence. Atlas carried the world on his shoulders. MM is hysteria fear porn which poisons mind and spirit. Mind control programs – be aware.
Your commentary is extremely uninformed. The population of the advanced western and Asian countries is declining except where immigration is present. Birthrates are rapidly declining everywhere in the world, although Africa less than elsewhere, even in relatively poor countries. The great long term problem will be how to care for the elderly. There will be less population on earth in 50 years almost assuredly.
Before presuming to call me uninformed, do a simple search on Google for the past year for India, pull out an inexpensive calculator, do the math and then perhaps respond. Thus far, every thing you’ve said is wishful thinking. Better yet, stay in your bubble- you’ll feel safer there!
Population will increase to around 2050 and then start to decrease quickly. Africa as pointed out is the problem. However with proper formal general education, population figures decrease
Ever increasing older populations are a real economic problem in most countries.
Mad Puppy, comparing early-stage death toll to Indian population growth is “not even wrong”. Outside of Wuhan, Milan and Madrid, COVID hasn’t even stretched its legs yet, much less gotten out onto field.
Data from Italy show COVID is now leading cause of death nationwide, and Francesco’s comment above says COVID has already matched the annual death rate in the towns hit early.
Unless you have some reason to think this pandemic will miss large chunks of the global population, the data show it’s on track to kill 1-5% of global population, depending on effectiveness of public health measures and access to medical care.
Only ways to reduce that are to slow it down (and pay an enormous economic price), accelerate a vaccine, hope an existing med actually works a meaningful amount of the time, or hope that the virus mutates into a less deadly form before it hits everyone. But hope is not a plan.
Wisdom Seeker; I cannot disagree with anything you’ve written. I wrote my first comment to only provide perspective and scale. The pandemic to date is small relative to world population, but certainly has the potential to grow beyond what one could reasonably imagine. One constant appears to be the limitations of our “leaders”. Brazil’s president calling the pandemic a ” small flu”, and India’s Modi having to apologize for abruptly shutting the country down and finding the poor migrants had decided to make their way back to their villages rather than potentially staying and starving in the cities for 3 weeks. One can’t just make this stuff up. I also heard Trump’s answer to the problem of restaurants suffering is to resurrect big business’ ability to write off food and entertainment expenses for income tax purposes. If that is ,in fact, true, that is as close to a “let them eat cake” moment as I’ve heard to date. I begin to wonder if I am on the same planet as a large swath of the American public!
Covered California (the state health insurance marketplace) has released a frightening memo on premiums for next year:
“Premium increases in the individual and employer markets for 2021 — which are in the process of being set right now — could be 40 percent or more solely because of COVID-19 costs in the absence of federal action.”
https://hbex.coveredca.com/data-research/library/COVID-19-NationalCost-Impacts03-21-20.pdf
If the insurance industry can’t handle a healthcare crisis without federal intervention, why do we need them at all? I think we don’t need the insurance industry in healthcare. Illness is not an insurable event because everybody gets sick. Insurable events are rare events.
In my part of Europe borders of the province with our capital has been shut down to slow down the spread to the rest of the country.
Police assisted by the military have established checkpoints to control traffic in and out of the province. External borders are closed, cinemas, cafés, restaurants, you name it, are shuttered. Take away is permitted, though.
Schools are closed, teaching take places as distance learning in the entire country. Streets are pretty deserted, it’s like on Midsummer Eve, then our cities are almost completely deserted, people being at their summer places.
Testing is mostly done only on those unlucky ones that are admitted to hospitals although there are testing points for those ordered to be tested. Apparently the case is that they haven’t got enough testing kits for this particular virus. Wartime readiness storages have been opened to supply hospitals.
Informatoin that seeped to the media indicates that there are 2 scenarios our authorities fear most:
A virusbomb at the western border and another one at the eastern border.
They fear that when health care will go on its knees in Sweden, Finns ( several 100k people) living there since decades, but still Finnish citizens, will start coming back to Finland and the authorities know that our healthcare will be unable to cope with such an influx of people.
They fear something similar in the east, too. They fear that migrants from St Petersburg and elsewhere in the east might begin moving west to escape the epidemic and the fear is that Russia might be in such bad shape that Russia will not have the will/capability to keep the border sealed. This was a very real fear when the Sovietunion did collapse, too.
The economic outlook is nasty, might even be that the early 90s will look nice in comparison and that was nasty times indeed. The longer the shutdown, the harder the hit will be.
Within New York State, the number of coronavirus cases per million population varies considerably, with counties in and around NYC reporting the highest numbers per million and much lower numbers elsewhere in the state. Westchester County is #1 with about 7875 cases in a population of just under 1 million. New York City’s 5 counties are less than 1/2 that, when adjusted for population.
Is there anyone left to count in the Bay Area? Seems every fourth car on the road here in AZ has Cali plates. ;-)
Has anyone here actually been tested? I was tested in San Antonio Texas on March 19 and the results were negative which didn’t surprise me since I had long recovered by the time I was tested.
What did surprise me was no identification was requested when I showed up for my appointment and I was notified by phone. So I have no proof of having been tested or the results.
Testing is completely haphazard and I have no doubt that we are only getting the tip of the iceberg when it comes to cases. My daughter’s family in Austin was told at the ER that they probably had it but they could not be tested. How many thousands like them are there?
While data and resulting charts are comforting in that we can quantify what’s going on has anyone considered that:
A. Test results are unreliable (but reliability/quality is increasing)
B. There’s a shortage of tests.
So, the equivalent of Non-GAAP financial reporting.
Mark, yes, I touch on the limits of testing in the text. I’d still rather plot tests than deaths. The data I really want to graph is the number of COVID-occupied, otherwise-occupied and “available” ICU beds per county or nation, which is something we could be tracking, but aren’t.
That’s a worthwhile approach. Do you know if anybody is tracking medical supply shortages generally, not just ICU beds?
@ Wisdom Seeker
I should have worded my post better. You did acknowledge the variation the the “Two Reminders:…” paragraph. I was trying to emphasize that in my opinion all data associated with testing is pretty much a low ball guess.
I bookmarked the COVID Tracking Web Site you linked to – Thanks!
@ Wisdom Seeker
addendum… graphing hospital bed occupancy is a great idea!
The shortage of resources available to US medical staff is acute and worsening. The official response to the pandemic was very late and federal help is still offered only grudgingly and with political strings attached.
Says one physician: “Unless hospitals want to burn through their doctors and nurses with us all in quarantine, they better let us protect ourselves.” Another added: “I’m not going into another room with a patient being ruled out for COVID-19 without an N95 mask. Period. They can fire me and the rest of the doctors and nurses who feel similarly.”
While it is true that the administration has not been successful in slashing the budget of the CDC due to congressional action, it is quite true that it has seriously defunded and damaged the US health ‘system’ at the federal level in other ways.
Since the inauguration, this administration has left almost half of US federal scientific leadership positions unfilled. In 2018, the CDC was forced to close or downsize its efforts to fight global epidemic outbreaks in 39 of 40 countries, including China. That same year, the administration dismantled the National Security Council’s global health security unit and recalled $252 million of emergency funds for rapid response to outbreaks. In 2019, the administration closed the US Agency for International Development’s program working with researchers across the world to respond to viruses.
The proposed 2021 budget released last month includes $3 billion in further cuts to core federal agencies including global health response programs, and at least some of those cuts are expected to pass even as the pandemic worsens.
That is on top of defunding at state and local levels in most of the country. The rich want to profit from health care, not pay for it, and therefore support politicians who then make the cuts to public health at every level. This has been going on for years.
In many senses the US does not have a public health system. Instead, medical professionals work in a for-profit healthcare system that is organised to maximise returns by minimising costs, making it easily overwhelmed by a national crisis. That system didn’t even work for medical professionals before the pandemic, and they had been quitting as a result.
As the pandemic spreads and they start dropping out in larger numbers – whether through frustration, fear, exhaustion, exposure, or death – the system will collapse, gradually, and the pandemic will increasingly run its course without their assistance.
@Unamused
“That system didn’t even work for medical professionals before the pandemic, and they had been quitting as a result. ”
—-
A decade ago I read a article about how financial reward sapped the spirit of the pro sports and increasingly, popular college sports. There was a trend to broadcast high school sports as a result. I’m not much of a spectator sports enthusiast so I’m not sure how that played out but I think the common point is that there’s a limit on the effectiveness of financial incentive. Maybe that’s obvious to this crowd. :-) I do believe there are those that will swim against any moment’s mainstream current intending to do the “right” thing.