Biotech stocks got crushed today, got crushed all week, got crushed since their peak in early July. “Bloodletting” comes to mind. But who the heck did the crushing? That’s what everyone wants to know. And the finger-pointing has started.
Early in the week, they blamed the New York Times because it had ran an article on Sunday on a hedge fund guy named Martin Shkreli who’d founded Turing Pharmaceuticals, which bought the rights to a generic drug that has been around for six decades, called Daraprim, “the standard of care for treating a life-threatening parasitic infection.” In his hedge-fund manner, knowing he had a monopoly, he jacked up the price from $13.50 to $750, raising the “annual cost of treatment for some patients to hundreds of thousands of dollars.”
This caused a national stink. Presidential candidate Hillary Clinton jumped into the fray with a proposal to cap prices of specialty drugs to prevent “price gouging.” Drug makers absolutely adore that kind of language.
Among the biotech giants, Biogen dropped 2.8% today, 9.5% for the week, and is down 40.6% from its high in March. Celgene plunged 4.8% today, 11.6% for the week, and is down 23.6% from its high. Gilead fell 2.3% today, 7.8% for the week, and 22% from its high in June. Smaller biotechs fared worse.
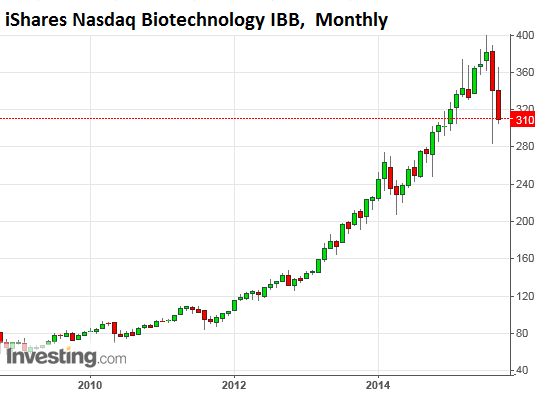
The iShares Nasdaq Biotech ETF (IBB) plunged 4.9% today, 12.9% for the week, and is down 22.5% from its peak in early July. This weekly chart shows just how bloody the week was – in percentage terms, the worst since 2008; in points, the worst ever:

But blaming the current drug-pricing scandals for the debacle? Thing is, these scandals have been going on forever. Sky-high drug prices are an old game. They explain in part why healthcare is approaching 20% of GDP in the US.
Even generic drugs are concerned. They should be a lot cheaper, but once competition disappears, such as in the case of Daraprim, “price gouging” is not uncommon. But it’s often not visible to the public because it happens to drugs used in hospitals. It disappears on confusing bills and ends up in higher insurance premiums and larger public expenses.
And among new drugs, we had hepatitis C drug Sovaldi, for which Gilead decided to charge $1,000 a pill. It was possibly the most “successful” drug launch ever. In the first quarter of 2014, Gilead sold $2.27 billion worth of the brand-new dug.
“We’re just looking at what we think was a fair price for the value that we’re bringing into the health care system and to the patients,” explained VP Gregg Alton in December 2013, after the FDA had approved the drug, and pricing triggered a media furor.
Fair for whom, exactly?
So let competition determine prices? Alas, the way it works, often there is no competition. And when there is, mergers and acquisitions see to it that competition doesn’t get out of hand.
One of the drug pricing scandals last year made it on “60 Minutes.” It involved Sanofi’s colon cancer drug Zaltrap, which cost $11,063 a month. It was a lot more expensive than Roche’s Avastin but wasn’t any better. So Leonard Saltz, a doctor on the show, framed the issue this way: “We’re starting to see the term ‘financial toxicity’ being used in the literature. Individual patients are going into bankruptcy trying to deal with these prices.”
And that sort of attention is unlikely to derail the momentum. On the contrary. When Gilead’s price of $1,000 a pill hit the headlines, its shares soared. It would be money in the bank. So something else must have derailed the momentum. Which takes us back to the biotech ETF.
How far did IBB actually fall back? All the way to where it had first been in December last year – so not very far. But look how the index ballooned since 2011. It went from 80 to 400. Doesn’t look like a bubble to me either:
Only a small number of companies in the index are even profitable. This leaves us with the suspicion that the real reason for the sudden swoon in the sector isn’t the vain threat of price controls, but the fact these stocks were some of the most glorious highflyers of the current era, powered for years by Wall Street hype, phony pro-forma projections, newfangled metrics, and day-trader momentum. They soared on volatile vapors. They didn’t need to be grounded in reality. This works for a long time – until suddenly it doesn’t.
It’s just one more phenomenon in the great Fed-engineered asset-price inflation game. It has spread to most other sectors, including commercial real estate, and the Commercial Mortgage Backed Securities that fund it. Read… Commercial Real Estate Shoots Off Chart, Fitch Frets about CMBS, Points to Financial Crisis
Enjoy reading WOLF STREET and want to support it? You can donate. I appreciate it immensely. Click on the mug to find out how:

![]()
This is what’s crushing bio-tech stocks.
Writing from a country (Canada) with a single payer health care system, that is on the verge of creating a country-wide drug purchasing plan to further lower the costs of necessary drugs, and as a cancer survivor who is off the surveillance program 5 years early, AND who has yet to pay 5 cents for any cancer drug or required surgery, I have one word to describe the US health care system and price gouging racket. “Criminal”.
(2014) “spending per person on health care remained highest in the United States (US$8,233). Canada was in the top quartile of countries in terms of per person spending on health, spending US$4,445; this amount was similar to those for several other OECD countries, including Denmark (US$4,464), Austria (US$4,395) and Germany (US$4,338).”
https://www.cihi.ca/en/spending-and-health-workforce/spending/canadas-health-care-spending-growth-slows
Health Outcomes:
Canada and the United States are similar in many ways, and until 40 years ago their health care systems were nearly identical. At that time Canada adopted a national insurance program (medicare). Simultaneously, the United States implemented its Medicare program for elderly people.
Although both nations continue to rely largely on private funding for drugs, they now differ substantially in both the financing and delivery of physician and hospital services.1 With respect to financing, Canada has virtually first-dollar, universal public coverage of hospital and physician services. With respect to delivery, not-for-profit institutions provide almost all hospital services, and large for-profit organizations are almost entirely excluded from the provision of physician services. In contrast, the United States relies on a mixture of public and private insurance to finance health care, and leaves 16% of the population without coverage. Investor-owned for-profit providers play a substantial role.
The United States also spends far more on health care, i.e., approximately 15% of its gross domestic product versus about 10% in Canada. In 2003, Americans spent an estimated US$5,635 per capita on health care, while Canadians spent US$3,003.
Paulo, glad to hear of you health success. Good for you. Not having to deal with the stress of how one is going to pay for critical health care is no doubt beneficial in one’s health outcome. You are almost correct, our healthcare system should be criminal, but unfortunately, it isn’t. I don’t expect the USA to always be as “exceptional” as many of my fellow citizens proclaim. But I do expect us to try to be.
Continued good health to you.
NT
According to this chart, the per capita spending on health care in the US is $4,221.5.
http://www.usgovernmentspending.com/US_per_capita_spending.html
Not that anyone knows the truth about USG spending. There are no real spending numbers. There are only made up numbers, just like the GDP numbers, with fake revised numbers later on.
Your fiscal data are well stated, however, you fail to address another key component: Access to care, even basic, well established care that is non controversial. The Canadian system is known in the northern tier of US states, and in the tertiary US referral institutions across the country as limited in access. Months for an angiogram, a year or more for a bypass, months for a joint replacement. Canadians regularly come to the U.S. and pay cash for services that are provided by their system, but not in a timely fashion. So, is cost containment accomplished by restriction and rationing of care? Is the solution to too much, too little?
I don’t know what country you are in, but I am in the US, and care is definitely rationed here by the insurance companies. Years ago when I needed an MRI I had to wait for 9 months for approval. A few years ago when my son need emergency dental surgery, he was in severe pain, I had to make hundreds of calls to the insurance company to get approval, it took over 30 days. Now the deductibles are so high that if you need care and don’t have the cash, you are F****D. I hate it when people pretend we have the best healthcare in the world, we don’t, we have the most expensive.
Just read this in the Miami Herald, man dies while waiting 18 hours for his ability to pay to be verified.
http://www.miamiherald.com/news/health-care/article36611469.html
The US healthcare industry is a wealth extraction machine. Criminal doesn’t sufficiently describe it, evil is a much better word. A system designed to impoverish the sick in favor of the affluent and rich can only be described as evil. A system designed to extract the savings of a lifetime because of an illness or accident is evil. A system that pretends to protect the elderly from ruin but instead codifies it, is evil. A system that promotes mutilation for profit is evil. Sometimes you have to call things what they really are!
Seconded. Health Insurance companies and their enablers in government are enemies of the very concept of human dignity itself.
My physician son readily admits that his charge rates would have to drop significantly if patients paid for their care, rather than insurance providers. I’d like to see if a free marketplace, that nasty word “capitalism”, would attract competition with its cost-reducing effect. Pols convince the populace that we need them to protect us, so we’re never going to wean ourselves off the dole ( our own wealth) dished out by those who are government Damning capitalism is a cheap shot fired by morally cheap people. I’m unaware of a non-socialist country on planet earth. Communism differs from socialsim only in substituting state ownership of means of production and distribution for the cumbersome manipulation required to extract from producers what they earn.
Hi JREwing,
Yes, there are waits….but the health outcomes are far higher than US results, and this is why.
Canada operates on the ‘triage’ system of access. The more critical your need, the faster you head to the front of the line. This is decided by the doctors invloved. Here are two examples. My neighbour had an indication of prostrate cancer. While getting his ct scan they discovered an embolisim in his descending aorta? He could die at any moment, apparently. The ct tech shut it down and called in a specialist. The neighbour was instructed to phone home and tell his wife he was going to undergo emergency surgery in Victoria, 3 hours away. They couldn’t fly him because of the condition so they transported him by ambulance and he was on the operating table within a few hours. In the US you have to have the money and insurance provisons to move to the front of the line, or at least to have the motivation to actually go see a doctor. I certainly accept that if you have gold plated insurance you have gold plated medical care.
5 years ago, on a routine physical I had a stange lump discovered by my family doctor. He arranged for an ultra-sound and a subsequent visit to a specialist. That took a month or two. I saw the specialist and he said to me, ” well, this has to come out. We are booked up in surgery, tomorrow. We will do it on Wednesday. I told him that was a problem for me because I was needed at work. He sat me down and said, “hmmm, sir that is a big problem. But it isn’t our problem, is it”? In both cases we went to the head of the line out of need, and not because of our connections or wallet.
If somebody rich wants to travel to the States and pay for immediate services, go for it. There are even some private surgery clinics in Vancouver that will happily operate as requested. But if you follow the system it usually works very well.
My neighbour had his operation and was saved. he had 72 staples down his front and looks like a zipper. When he recovered he went backl to the urologist who prescribed howmones to shrink his prostrate down and booked suregery. (He was unable to have radiation due to prior treatments for another condition, years ago). Anyway, they removed thee prostrate and he is cancer free to this day. This same guy had 1 tripple bypass years ago, treatment for colitis, plus the two mentioned surgeries. He is now 75 and is still going strong. He was a bridge builder superintendent and his past taxes paid for his subsequent care when he needed it.
Oh yeah, his costs for all of his medical treatments? Zip.
In my life I have had broken legs, ruptured appendix requiring surgery and drains etc, herniated discs, knee operations, and cancer surgery. When the oncologist reviewed my records she wryly asked, “any other bits and pieces missing”? (I live a pretty active life). My costs for the treatments? Nothing.
We pay higher taxes and more for our booze, etc. However, it is a bargain and wonderful not to fear bankruptcy or house loss due to health problems.
regards
Well put sir. Bile rises the the throat when I hear the “but you might have to wait for non-urgent care!”
All I hear when that argument gets trotted out is “I’m not poor, and my convenience trumps your survival and ability to live with dignity.”
This is an excellent discussion. I’m glad we’re having it right here. It’s good to hear from our Canadian neighbors about their system, pros and cons.
It strikes me that the issue of ostensible price gouging, by the actual R&D developers and product producers, is being given exaggerated focus, while glossing over the exploding costs for directly and indirectly related government-bureaucratic expansion and waste. This discussion explores some convincing rationales for “single payer,” basic healthcare and hospital services, but fails to address the bottom line aspect of critical R&D spending, for which no amount of government structured, bureaucrat controlled research will realistically compensate. It seems obvious that the American model, and based, biotech industry, and its related international collaborators (Celgene is one good example), is providing most of the significant innovation for cures for complex illness, and in which one thing, essentially and eventually, leads to another… Some “cures” may well start out very expensive, but lead to potentially dirt-cheap solutions, by comparison, several decades later, not unlike new drugs transitioning to generic. Virtually no significant innovation, in these regards, is coming from the socialist/left, totalitarian and other third world.
Also, the cost for nursing home and related maintenance services is exploding with the reality of demographics. Aren’t costs for these services, as well as public healthcare for the understated, illegal immigrant invasion (what it is), actually being “redistributed” into the larger billing structure? I have to be skeptical that reasonable, even incentive driven profits for the extraordinarily hard-working doctors, their irreplaceable colleagues, and critically important R&D investors, combined with fairly, but modest profits (by comparison) for the essentially only administrative insurers, are the significant problem.
Love your commentary Wolf!
Setting aside for a moment the question of single payer US vs Canada, two meaningful reforms we could adopt in the US would be to 1) ban differential pricing; and 2) force “one price” billing.
Regarding #1, a health care provider would have to charge all patients the same amount for the same service, regardless of insurance status. For example, I had a routine preventative procedure late last year. It was covered by insurance, which paid the hospital $1,400. However, the hospital’s “sticker price” was $18,000, and if a person was not insured and the hospital smelled money, they would pursue that individual for the full $18K until the end of time.
#2 would reduce complexity and allow patients to compare prices more readily. If we paid for computers the same way we now pay for health care, we’d get a bill from the disk drive manufacturer, another one from the motherboard manufacturer, dozens of others from other component manufacturers and a final one from Dell for putting the whole thing together.
Stripping out complexity and improving transparency are the only ways we can reform this monstrous system. Sunshine is indeed the best disinfectant, which is why the people profiting from it are so resistant to allowing it in.
You are delusional if you think the system we now have can be improved by changing a few basic flaws. The entire system has to be shut down and restarted as a non profit single payer system. The system cannot be reformed, because as long as it is a profit center for the economy, it will be manipulated by the politicians for bribes. We are being extorted by the healthcare industry and the politicians are on their side. Trump coming out in favor of a single payer system is the reason people are supporting him and looking the other way on many other issues.
Back in the late 1980’s – early 1990’s I was privileged to live in Buffalo, NY and my job took me to the Canadian province of Ontario on an almost weekly basis. During those years I learned a lot about the great Canadian people, and had many an after work discussion of the perceptions of each about the other.
One of the things I noticed was the universal rejection of the American healthcare model over the Canadian model. Yes, theirs IS the better idea – BY far! The cultures are hardly identical, but yet remarkably close. Probably much closer upon a detailed inspection than either group may wish to admit.
One of the great failures of the “Obamacare concept” was the refusal to have a publicly funded aspect, and the exclusion of both dental and vision. Both of these could be corrected by the expansion of medicare to all. Yes, we would need to do some tax funding here via “sin” taxes, and probably petroleum, which they claim is destroying life on the planet anyway. Yes, it is well past time to take a universal like healthcare, prescription drugs out of the capitalist model, and away from electoral politics meddling like allowing medicare to negotiate drug prices.
Actually so much needs to be re-though here, and with our elected leaders cannot pass a ‘simple’ annual Federal Budget each year, perhaps there is NO hope.
Well, we can at least say we are all to aware of their constant failures, and my hope springs eternal we might replace the defectives.
As an American living deep in the heart of NYS (about 50 miles outside Manhattan) I can attest to Paulo’s description of the Canadian health care system’s triage of access: my wife’s niece is married to a Canadian, and his aging parents may have to wait for certain routine, but non-life-threatening/lifestyle threatening, type care. But when his dad needed knee replacements (both) and his mom needed (and needs) treatment for macular degeneration, the procedures and treatment were/are available in absolutely timely manner with minimal out-of-pocket costs (as in hundreds of dollars). As appropriately commented above, without a generous (and very expensive) health insurance plan here, approvals from PCPs and more if you have to go up the ladder can take weeks and months, not to mention the frustration and anger in dealing with non-responsive customer service personnel, the “better” ones who are paid more to stall and filibuster in the best tradition of US politicians. JREwing, take some time to do some due diligence before harping on what you know little about.