Under onslaught of new competition, monopoly status collapses.
Mylan’s EpiPen – the center of one of the many blistering scandals on Big Pharma price gouging – is getting hammered in the market, as competitors have burst on the scene, and as health insurers and prescribing physicians have gotten the memo. Its market share plunged from 95% to 71% in just two months!
Mylan had acquired the rights to the decades-old product in 2007. At the time, pharmacies were charged less than $100 for a two-pen set. By 2009, pharmacies were charged $103.50 for a set. Then the annual price hikes set in – “peaking every year in August, when parents of children with severe allergies typically stock up on the life-saving devices for use in schools.”
In 2016, the price spike hit $608.61 – an increase of over 500% in a decade. And this finally kicked off the uproar that landed Mylan CEO Heather Bresch on the hot seat before the House oversight committee hearing on EpiPen price increases.
Though the medication (epinephrine) is decades old, it is delivered by patent-protected auto-injectors, which allowed Mylan to get away with price gouging for so long.
In December, as a result of the uproar, Mylan introduced a cheaper generic version of its own product to appease the unruly riffraff having to pay for it, and more importantly, to try to protect its market share against the onslaught of new competition. And EpiPen’s world of easy mega-profits is changing.
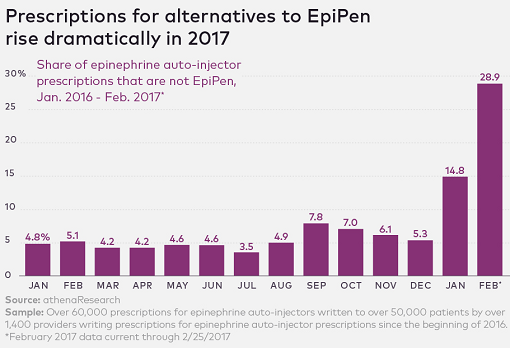
A report by athenahealth that analyzed more than 60,000 prescriptions for epinephrine auto-injectors by over 1,400 providers across the country between January 2016 to February 2017 found that “with no generic versions of the lifesaving allergy medicine, and few comparable products on the market at the time, the vast majority of physicians were not prescribing alternatives — until now.”
Auto-injectors that compete with EpiPen have started to tear into EpiPen’s market share in January and February. In December 2016, the market share of the EpiPen alternatives was still 5.3%. By February, just two months later, it had more than quintupled to 28.9% (via athenahealth):
The report wonders, “Why the sudden shift?” Part of it has to do with insurers that are getting smarter. For example, in January, Cigna started covering only the generic options to EpiPen.
And then there’s the rejuvenated market for these products:
Patients and providers might be reaching for the alternatives and generics that have recently hit the shelves, as the industry responds to widespread demand.
Generic options captured in the data include Mylan’s own EpiPen alternative, at half the price of the original, which the company released in mid-December. Kaleo’s AUVI-Q was re-released in mid-February, and CVS recently announced that it will stock Adrenaclick, a $10 EpiPen alternative.
A $10-alternative (it’s actually $110, but is offered with a $100 manufacturer’s coupon) to a decades-old product that costs $608.61! That’s the signature of price gouging, carried out on the backs of consumers that have to pay for it either directly, via insurance premiums, taxes, or a combination.
The perpetrators such as Mylan – and there are many other pharmaceutical companies engaged in similar strategies, protected by lobbying, patent laws, consolidation, and inscrutable pricing strategies – have become Wall Street heroes. PE firms have muscled into the money-maker to wring out those that pay for it, even as allegations of collusion and price-fixing have become rampant.
It’s an all-too rare thing that public pressure, short sellers with a big megaphone, and uproar in the media – however feeble and ephemeral they may be – are able to crack open the artfully erected constraints in the healthcare market, what little there is, and allow competition to fix the problem.
Another money machine appears to be running out of steam after providers of the S&P 500 and MSCI indices suggested that they might not include Snap’s just issued shares into the indices due to their non-voting nature, which is deflating a big part of the extraordinary hype around what had been the hottest tech IPO in three years. Read… Investor Group Attacks Snap’s No-Vote Shares, Stock plunges
Enjoy reading WOLF STREET and want to support it? You can donate. I appreciate it immensely. Click on the mug to find out how:

![]()
But isn’t this how it is supposed to work in our current system: get a patent, get people hooked because you are the first to cure/subdue disease, raise prices like crazy, make out like a bandit before the patent expires? It shouldn’t be shocking that generics will eventually take over and this does little to really deter people from this behavior. No one cares about the company lasting forever aside from the workers.
Kit
Well, if there’s zero incentive to create new drugs, you’re gonna get no new drugs. You can’t have “generics” until the patent expires.
Of course, you could have the Federal government perform all drug research (JUST KIDDING! We already tried this with Tuskegee and syphilis, the US Army & LSD…).
A more productive question is where are the regulators in all this? Even if this isn’t technically illegal, public shaming of these drug organizations is very effective.
…and another couple of things:
1) This stock (MYL) is only down 10% in the last 6 months.
2) YIKES! This stock has a PE of 87! Once these guys begin to miss earnings, this could fall like a cement canary.
Where’s Bill Ackerman & the shorts when you need ’em?
If they bring back over the counter rescue inhaler, Primatene Mist, then I will know the days of Big Parma price gouging are numbered; which they should be as this model is not sustainable.
Agreed-I used to use the Primatene and now use the clumsy AsthmaNefrin inhaler. It’s a lot more expensive (although significantly cheaper than the prescription Albuterol the medical cabal wants used) and clumsy. The excuse was that doctors weren’t involved with Primatene so they first used the idiotic damaging the ozone layer originally and then blocked replacements that did not use CFCs to prevent another non-prescription replacement.
There were CFCs on old inhalers, but the amount really didn’t matter. Pharma pushed to have them banned because newer ones had patent protection.
http://www.motherjones.com/kevin-drum/2013/10/heres-why-your-asthma-inhaler-costs-so-damn-much
I taught school for 17 years in BC and have never ever heard of someone not being able to afford several epi-pens to be kept on site. The student always carried hs/her pen with them to have on the playing fields, game days, or for field trips, etc…and the school office also had a supply of pens. Teachers received instruction on how to use them. Students that did not have a supply of required medications would not be allowed to attend certain activities.
In our single payer system (BC Canada) the attached quote is our policy to keep drug pricing down. In our family’s case we also carried Blue Cross for extra health services which in turn pays for everything after a certain threshold has been reached. It has now been folded into a plan called Green Cross. We carry this coverage because my wife is type 1 diabetic and has been for 50 years. For her entire cost of supplies we pay approx $300/month, but this also includes my coverage, our dental plan, eyeglasses, BC Medical Plan, etc. For low income citizens there is a pharmacare plan that pays for prescriptions. This is the policy to keep down the costs to taxpayers:
“Low Cost Alternative Program (LCA)
PharmaCare’s Low Cost Alternative (LCA) program helps control the cost of prescription drugs. When the same drug is made and sold by more than one manufacturer, PharmaCare covers the less costly version—the low cost alternative.
How is the maximum price for drugs in the LCA program set?
PharmaCare creates a separate category for each type of drug based on its active ingredient, its strength and its formulation (tablet, capsule, etc.). For example, there is one category for acetaminophen 250 mg tablets and another category for acetaminophen 500 mg tablets.
PharmaCare sets a maximum price it will cover for each category based on a percentage of the price of the brand name drug. If a manufacturer wants its generic drug included on the list of LCA drugs that PharmaCare covers, it has to agree to sell the generic drug to pharmacies at or below the maximum price.
PharmaCare covers the drug up to the maximum list price plus a fixed markup for pharmacies (usually 8%).
How does the LCA program benefit me?
The LCA program helps you in two ways:
Saves taxpayer dollars and helps PharmaCare continue covering a broad range of drugs for you and all B.C. residents.
It helps you pay less for your prescriptions. If you pay part of your drug costs out of your own pocket, the lower the overall cost, the lower your portion of the cost will be.”
This is a pretty informative and interesting link to how the BC medical Plan works.
http://www2.gov.bc.ca/gov/content/health/health-drug-coverage/pharmacare-for-bc-residents/what-we-cover/general-coverage-policies
regards
“We carry this coverage because my wife is type 1 diabetic and has been for 50 years. For her entire cost of supplies we pay approx $300/month, but this also includes my coverage, our dental plan, eyeglasses, BC Medical Plan, etc.”
You poor, poor, yet gallant Canadian bastards. I am betting your deductible must be somewhere near $5,000 and total annual out of pocket in the range of $20,000 at that monthly rate.
And I only have to wait a couple of months to see my dentist. From what I hear you guys have to wait years.
I dont know if you are serious about the wait times for seeing a dentist in Canada but my wait time is 1 – 2 weeks with or without insurance.
I sense deep dark sarcasm in Kent’s lament.
Kent,
Chill your anger, boyo. We are a democratic country that pays (taxation) for its own decisions made at the ballot box. Our system works. Yes, it has many many problems, but what doesn’t that tries to address so many complex and compounding issues?
I watched Sean Spicer touting the new and wonderful Trump-Care Obama-Lite plan while I ate lunch. Then, I saw the GOP diehards saying they want to repeal everything…right now. All I thought was, “Why don’t US citizens just get what their congress and senators get”? I mean, my MP and MLA get the same health care coverage that I receive. Isn’t that fair and just? Hell, our Prime Minister gets the same coverage as my family. If he paid for private care and a line budge he would be voted out next election cycle.
We pay higher taxes in Canada which provides these services. People usually don’t mind paying taxes when the results directly benefit themselves and their families as opposed to the US insurance cartels and private hospitals.
Sorry, there is no deductible charged to me at source, or co-pay for my medical coverage. THAT is the cost. I pay 20% for some of my dental work.
I just went to the dentist last week. It took me a week to get my appointment for a checkup and cleaning that suited my schedule. (I live in the boonies and only go to town once per week). I think my Dentist has a degree from McGill. My Hygenist has a degree from UBC. Both of these universities are world class.
Last week I went to the Doc to get a hayfever prescription renewed for the next season. An appointment that suited my schedule was available in 3 days. Or, I could go to the clinic’s walk-in service the same day, which might require a 10-30 minute wait. My bill for the prescription re-fill? Nada. Or I should say it is covered by my $300 monthly supplemental Blue Cross.
I have had cancer surgery, many follow-up ct scans for surveillance and have subsequently been released from the system as cancer-free. Cost to me? Zero. Knee surgery? Cost to me? Zero. Herniated discs (all this stuff work related) Zero. By the way, my cancer surgeon was also educated at McGill.
I don’t get your hostility. US citizens need to insist their politicians implement single-payer. We did it in the ’60s. There was a ballyhoo whine from the medical industry plus a doctor strike in Sask, but no one complains about it anymore except for those few specialty surgeons with their own clinics and private wealthy clientele. They have subsequently been denied from using public facilities because they charge additional fees above and beyond the rates set by BC Medical Plan. (The private practice doctors, not the patients are denied hospital priv.) Your insurance cartel will shout the sky is falling, but health outcomes will improve at 1/2 the cost for your country as a % of GDP. Of course that would be socialism, and socialism only applies for the banking industry and multi-nationals. Right? :-)
Two things to consider:
“A recent Brown University study, for example, pinned the cost of the wars in Iraq, Afghanistan, Pakistan and Syria at about $3.6 trillion from 2001 to 2016, using the $1.6 trillion operations costs as a baseline but also accounting for counterterrorism costs.”
http://www.politifact.com/truth-o-meter/statements/2016/oct/27/donald-trump/did-us-spend-6-trillion-middle-east-wars/
And:
Health care in the United States is provided by many distinct organizations.[1] Health care facilities are largely owned and operated by private sector businesses. 58% of US community hospitals are non-profit, 21% are government owned, and 21% are for-profit.[2] According to the World Health Organization (WHO), the United States spent more on health care per capita ($8,608), and more on health care as percentage of its GDP (17.2%), than any other nation in 2011.
Plus:
In 2016, total health expenditure in Canada is expected to reach $228 billion, or $6,299 per person. It is anticipated that, overall, health spending will represent 11% of Canada’s gross domestic product (GDP).
Finally:
Recent statistics estimate Canadians born in 2007 can expect to live to 82.3 years for girls and 79.3 for men, compared to 80.8 and 75.6 for kids in the U.S., respectively.
regards
I believe a Republican congressman today said that people could afford whatever new healthcare system is coming if they’d just give up their iPhones.
The rest of the world reaps the benefits of Americans’ paying too much for pharma/medical products.
Whenever there is “price gouging” it comes from lack of competition. Price controls work- only in the short run. Competition always works, but sometimes competition is purposely prohibited, e.g. by patent (= monopoly protection). Patents have to be sensible; Epipen patent is a good example of a nonsensical patent.
If the parts of the system are not implemented correctly, you get what happened here.
Minimize patents, inject competition and as much free market activity as possible, and you will solve these pharma pricing issues.
Sensible regulation/patent, etc. are part of the requirement. The government has to be a competent referee, not a player in the game.
Paulo-
I also live in Canada. As much as you are right about a bunch of things in your post, you are quite wrong about the MPP’ MP’s and PM getting the same healthcare as the rest.
Officially, we have single tier healthcare in Canada, but in reality we have 3 tier.
The bottom tier is for all the hoi polloi.
The 2nd tier is for those who know insiders.
The top tier is for those both well connected and with lot’s of money.
There are lots of private hospitals and private healthcare providers in Canada. They just aren’t talked about.
In Toronto alone, if I have the cash, I can walk into the Cleveland Clinic and get any sort of world class treatment, without waiting in line. That’s just one of many choices. Vancouver will have a number of them as well. Who do you think treats all the sports stars, actors and rich Asians?
You can damn well bet PM Trudeau isn’t going to the local hospital for a checkup.
That’s because the Canadians are our moral superiors. One hears this every time we discuss why our murder rate is so much higher than Canada’s, and it probably explains why their health care system is better.
“I believe a Republican congressman today said that people could afford whatever new healthcare system is coming if they’d just give up their iPhones.”
Yeah, I’m sure giving up $700 iphones and Droids will enable people to finance $250,000 surgeries and chemo treatment. Presto! Problem fixed.
The BC plan like all Canadian plans have very small deductibles and no co-insurance. Waiting times are very similar to US experiences depending upon where you live. Its a very good system and very reasonable costs. Trump had considered a similar plan for the US . Its the only way to go to achieve anything like universal health care. First step is to combine the VA, Medicaid and Medicare systems into a national system that anyone can get coverage and subscribe to.
Kent, could you clarify if you were being sarcastic?
Some readers are taking it seriously, but I think there was an invisible /sarc tag somewhere.
I apologize, I was being sarcastic and left off the tag. Worse yet, I ran off and never came back. Won’t happen again.
But he did call us gallant and bastards. I’ll accept the praise. ;)
One of the funny things is that you will rarely see Canadians complaining about their health care, or the cost of their health care. They take one quick look south and thank their lucky stars. The american system is to put it mildly … uncivilized … as are the “discussions” to try and “fix” it.
Off on another tangent … for the single payer folks … What would be a great idea would be to have the countries with single payer systems combining to undertake research for drugs/treatments that pharma’s won’t touch because they can’t make any money on them. It would be in their collective interests to find more medically effective and cost effective treatments – ones that would never see the light of day with Big Pharma. Would seem to be an excellent investment.
Well said, your last name is truly fitting. But it unfortunately appears many will suffer in the US before we can even consider your interesting tangent. I will try to add another “funny thing” about big Pharma. Other than that the flush toilet and septic systems have done far more than they EVER will to increase lifespans.
Plus the discovery of bugs! Thank Louie P, not those pill-pop promoting jerks.
Since they all run such IMMENSE Rx drug advertising budgets, (probably way more than OTC which you can just go buy and try any old time), do they feel ALL our Docs are not very “aware” of new pharmaceuticals and they want to give YOU, who know NOTHING, a way to HELP your Doc do his job better? OOOOK……
In FACT, when I dropped out after completing the first (of 3, the last yr being more of an internship) professional year of Pharmacy at Oregon State in 1979, the “detail men” as the drug salesmen from the companies who visit the Docs are called, were costing companies around $3K/yr/Doc. A good one could make $75K/yr. Way more drugs out since then. I’d hate to think what the total budget for advertising is now. They didn’t advertise on TV then.
Why did I drop out? Ethical reasons. WE have had some drug winners, no DOUBT (oddly enough one of the BIGGEST by a “poor,poor” Canadian, btw) but most of it is pure BS. They have us all believing in “take this for that”. Well “this” may do ‘that”, but it also does tens of thousands of things they don’t know about. Without getting into the complexity of bio chem, let me put it this way:
Nature has had 3 BILLION years to experiment with living things….do you honestly think the timescale of a MERE CENTURY of the same by us amazing humans is going to make so many MAJOR improvements?????????
The BIG improvement EXCEPTION being our amazing “body mechanics” as I call them. Doctors. They have always preferred “Physician” themselves, which is closer to my notions of hands on Science devotees. Especially everyone involved in surgery, actually re-plumbing you, replacing parts, rebuilding moving parts, etc.
Those guys totally amaze me, and their skills and progress of same have my respect, including the unsung GP, who has to point you in the right direction, with all the possibilities he has to consider.
And especially the ER BUNCH.
Pharma would, if they were less greedy, and maybe had to face a patient in anaphylactic shock from their junk…back to the Epi-Pens….
Plus my Dad was a Doc…the real old time kind…made house calls.
My son was born pre-mature, a month early , here in Calgary- Alberta. He spent a month at the Neo-natal intensive care unit at the Alberta Health Services.
We did not pay a single dime. They gave mother and child, the best care possible.
We do not have a perfect system, but we do have a humane system. I am more than happy to pay more than my share of taxes to ensure all Canadians (regardless of race/culture/sexuality) have lifelong access to the same healthcare we received – and this trait is what makes us Canadians.
My son is 5 years now, and he wants to be a doctor – here in Canada.
The entire CCC (Criminal crony capitalists) sick maintenance and pharmaceutical industry is rife with rackets designed to extract maximum fees from patients, employers and government. Obamacare was always intended to greatly increase the profits of the CCC (Criminal crony capitalists) “healthcare” and pharmaceutical CONporations.
An example are painkillers. Endorphins are the human body’s natural painkiller. The pharmaceutical industry has developed artificial endorphins. But, natural and artificial endorphins are not addictive. Nor does the body develop a tolerance to them that would require ever increasing doses like other pharmaceutical industry painkillers. The CCC (Criminal crony capitalists) pharmaceutical industry suppresses the commercial availability of artificial endorphins to maximize their profits from highly addictive and deadly drugs like morphine, heroin, fentanyl, codeine, oxycodone, OxyContin, etc. The United States of America’s Feral Gangster Government is Complicit in the crimes of the CCC (Criminal crony capitalists) pharmaceutical industry.
In the United States doctors are either bribed or blackmailed to write prescriptions for the most expensive drugs and to shun inexpensive generics. My doctor insisted on giving me a prescription for a less effective, more addictive brand name drug costing $550 per month. He refused to write the prescription for a less addictive prescription more effective generic that would have cost maybe $10. Unfortunately, I can’t afford to pay $550 per month for 1 prescription. So, pardon me if my feelings about the CCC (Criminal crony capitalists) pharmaceutical CONporations aren’t loving kindness.
If you have Kaiser insurance available in your area, I suggest you consider it. The doctors have no incentive to prescribe expensive advertised drugs when there are less costly choices available. I can’t remember paying more than a $10 or $15 co-pay for any prescription I have ever had to use. If the US is ever to fix its grossly expensive medical care system, Kaiser is the way to go.
Both the Canadian and US medical insurance system have their pluses and minuses. Every Canadian has had a medical insurance card since January 1, 1966. No one is bankrupted by medical bills in Canada. But sometimes people die waiting for specialized services such as heart surgery. Google Jerry Yanover. He died in Ottawa waiting for his scheduled surgery in the summer of 2009. I remember reading his online obituary when he died.
It is deceptive to look at the differences in life expectancy in the two countries and then blame them all on the US insurance system. That leaves out the many problems in US ghettos, including their very high homicide rates, as well as the limited access to medical care for the many illegal aliens in the US. But I suspect that the average poor American would fare better under the Canadian medical care system.
great job, once again, Wolf. thanks for your insights!
Tell me why the CEO is not in jail?? Hopefully she rots in he** and has a bad case of stomach flu today!!
Another overlooked cost difference between USA and Canada systems is malpractice insurance . Premiums are brutal in U.S. vs virtually non-existent in Canada due to the difference in tort laws. Good luck suing a doctor in Canada and getting a multi million dollar lottery winning for a botched hang nail operation.
In addition, doctors’ charges for various procedures are negotiated / imposed by the various provincial governments but generally lower than in the U.S. due in part to the above insurance.
“A $10-alternative to a decades-old product that costs $608.61!”
=========
I’ve just done a cursory search for that $10 product “Adrenaclick”. I can’t find it for under $100.
$10 is the price pharmacies pay, according to the report. Just like $608.61 is the price pharmacies pay. What you pay ends up being a more complex matter, depending in part on what your insurance negotiates, etc.
The real test would be to walk into a pharmacy with a prescription and see what it will cost, cash price and at the insurance rate.
On further checking…. Yes. It’s $110, but is offered with a “$100 manufacturer’s coupon,” according to the report. Hence the $10 the report uses.
That coupon part slipped through my fingers. I have meanwhile updated the report. Thanks for pointing it out.
Nearly 1 in 10 Americans has diabetes, so it should be obvious that self-administration from vial of generic epinephrine, using the same technique and small syringes that diabetic use, can be done almost as quickly as using an Epi-pen that costs over 100x as much per dose. The question is how school nurses, other health care professionals and the public were ever in effect blackmailed into accepting systematic price-gouging in the first place.