By Michael Gorback, M.D., board-certified in Anesthesiology and Pain Medicine. He taught for 8 years at Duke University and is the author of 32 scientific articles and textbook chapters, and one medical book. Dr. Gorback currently practices pain management at the Center for Pain Relief in Houston, TX, and claims that nobody has ever suffered due to lack of knowledge of his opinion.
This article is a WOLF STREET exclusive.
The most heated discussions in healthcare revolve around “pay for performance” (P4P), a nebulous term that generally entails a system of financial incentives to doctors, hospitals, and other providers of health care services to improve care in some fashion using “measurable” outcomes. Studies have been run with mixed results. Systems have been debated ad nauseam. But one parameter – indeed THE basic parameter upon which P4P is based – “pay,” is more than a little hard to quantitate.
Someone recently criticized me online after reviewing my Medicare billing data. This information is now published online by Medicare, with the latest data being from 2012.
The two main criticisms were (1) that my charges were about 50% higher than average among my peers, and (2) that I did three times as many procedures as my peers. Here is a screen capture of the data:
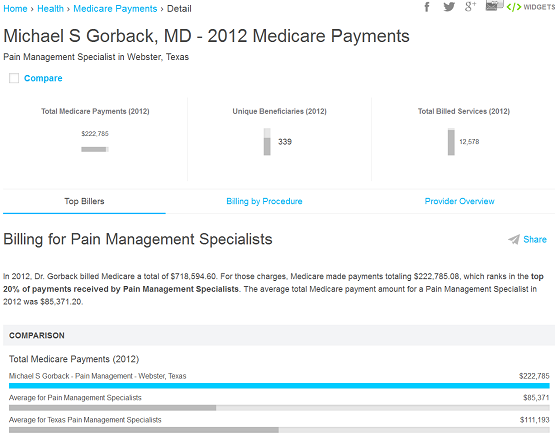
Looks pretty unflattering. Screen capture #2 shows the two highest costs of my practice for Medicare. This is about half of what Medicare claims it paid me.
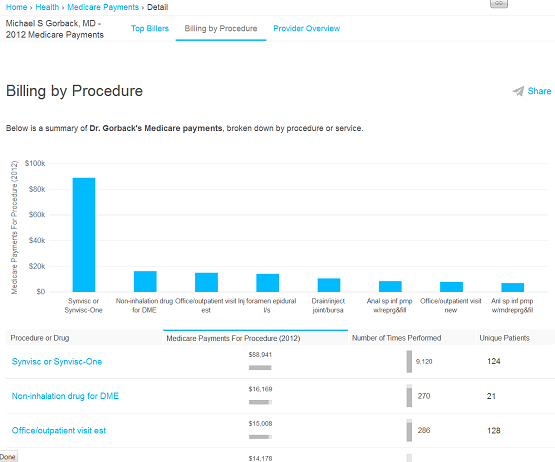
The #1 line item was “Synvisc or Synvisc-One.” This is a drug that is injected into the knee to treat arthritis. Medicare seems to think that doctors obtain and store medication at zero cost so there is negligible markup. Medicare pays me roughly enough to cover the cost of the drug. Don’t you wish your favorite restaurant was prohibited from marking up the alcohol and could only charge their cost plus a fee for serving it?
So $89,000 of the reported $223,000 payment was just recovering my expenses. This is not what I get paid for performing the injection.
Let’s look at line #2, “Non-inhalation drug for DME.” This had me stumped for a while. DME means “durable medical equipment.” But what was this “non-inhalational drug” business? It turns out that’s what Medicare paid for the medication that we use to refill implanted pumps for management of severe pain. Once again, Medicare doesn’t think we should be able to mark this up.
So now we have $89,000 + $16,000 = $105,000 that was merely reimbursement of costs, or almost half of the reported payments they made to me in 2012. Some pain specialists manage pumps, some don’t. I would wager that few do as many Synvisc injections as I do because I get a lot of referrals for this from orthopedic surgeons who don’t want to do them.
How did I manage to perform triple the number of procedures? Once again, the answer lies in the Synvisc. According to Medicare, I did over 9100 injections on 124 patients. Whoa! That is some serious activity – over 1500 hours of knee injections in one year assuming I could turn them over every 10 minutes on a conveyor belt! That’s over 180 8-hour days if I don’t break for lunch and manage to control my bladder.
This is an artifact produced by the way Medicare pays for Synvisc, which is per unit. A single syringe of Synvisc One – enough to inject one knee – contains 48 units. We divide 9100 by 48 and discover that I only administered 190 syringes of Synvisc One, distributed over 124 patients. Some of these represent bilateral procedures done at the same visit, while others represent repeat single injections (Medicare pays for repeat Synvisc One injections every 6 months).
There’s quite a difference between 9100 procedures and 190 procedures. The way Medicare presents this improperly inflates the number of procedures reported.
Here are some comparable data from a colleague who practices near me. I happen to know him well and I respect him both personally and professionally. His Medicare collections in 2012 were roughly the same as mine.
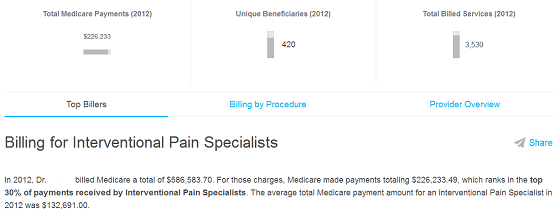
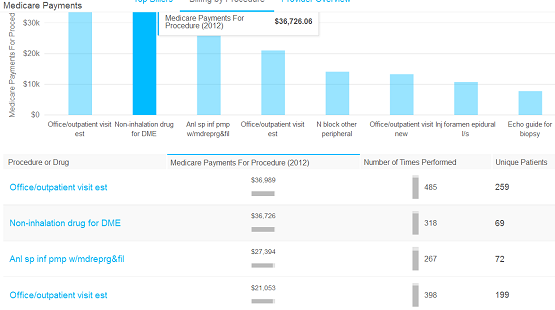
Note the absence of any Synvisc. His pump medications ran about double mine, probably reflecting more patients with pumps than I have in my practice.
Unless the subsequent lines represented a lot of cost reimbursements, this doctor netted a lot more from Medicare than I did. Somehow despite collecting more than I did, he was ranked in the “top 30%” and I was ranked in the “top 20%.”
The government, amongst others, would like to have us change to some form of “pay for performance” system. Unfortunately, they can’t even get the most basic metric – pay – correct. From the people who brought you healthcare.gov.
The easiest way to implement pay for performance is a free market. Free markets serve as large information exchanges, constantly updating price and value. In a free market system, good doctors with satisfied patients would command greater prices. To think that some central government entity can more efficiently determine prices reflects a pathetic misunderstanding of the way the world actually works. By Michael Gorback, M.D. at the Center for Pain Relief. This article is a WOLF STREET exclusive.
Also by Dr. Gorback: Bookies call it the “vig,” insurance companies call it a “PPO Repricing Fee.” It allows them to go around state insurance laws. Read… How Hospitals and Health Insurers Collude at Your Expense
Enjoy reading WOLF STREET and want to support it? You can donate. I appreciate it immensely. Click on the beer and iced-tea mug to find out how:

Would you like to be notified via email when WOLF STREET publishes a new article? Sign up here.
![]()
Sorry to contradict you. Medicine in all its aspects is a typical example of an asymmetric information system, in that the patient knows a lot less than the doctor, making it possible for a doctor (not you, of course) to sell something different than the patient thinks he’s buying. Like estate agents and second hand car dealers.
So the US has had this free market in medicine all these years and as a result has one of the highest percentage of its GNP spent on medicine in the OECD countries and a lower life expectancy than in most of them. Yes, the free market works, but it doesn’t always work efficiently.
That’s incorrect. We have had a private insurance system in effect for decades, as well as Medicare and Medicaid. All of these programs insulate the consumer from the cost, thus breaking the price discovery mechanism.
The doctor has asymmetric knowledge but the patient ultimately makes the determination as to the value the physician brings. This gets disseminated among the consumers of health care services by word of mouth. The feedback also affects other doctors. If I refer you to someone and the experience is good that doctor gets more referrals from me and vice-versa. I want my patients to have good care. Additionally, a referral that goes badly reflects on my judgment.
As for the data, doctors can only compensate for had habits so much. We can’t make you diet, exercise, or stop smoking. We can nag but we can’t follow someone home and make sure they take their insulin or spend a little time on the treadmill. In areas where doctors have more direct control, such as cancer, we kick ass.
Doctor,
I doubt that doctors, hospitals and pharmaceutical companies want the price discovery system that would exist without private insurance, Medicare and Medicaid.
I grew up in a time when none of these existed. When my younger brother was born my parents price shopped for a hospital and thought $125 was exorbitant, but the best that they could get. No one could convince them that one hospital was superior to another for the service they wanted because my mother’s pediatrician was the one who would deliver the baby.
My mother would haggle with doctors. She would object to a $2 charge for an office visit on the grounds that the doctor 2 blocks away charged only $1.50 and threw in the medicine for free. She believed $2 was fair for a home visit.
I think the entire industry would definitely prefer to have their lobbyists negotiate price with government. Government is a lot freer with the public’s money than each individual consumer would be with his/her own money.
You only think a free price discovery mechanism would be good until you discover the price.
You’re absolutely right NY Geezer. If there were no third party payers there would be massive deflation in 15% of the economy. The longer you let a dislocation fester the harder it is to undo. Now we’re at a point where people think it’s impossible to have a system without third party payers and a rigid regulated pricing system.
Because the USSR and Red China worked out so well, right?
Health care is unique in that unlike most goods and services there is a general societal sentiment that cost shouldn’t be a barrier. We don’t want anyone to suffer from illness just because of the money.
OTOH, if cost is not a barrier costs become hard to control. Then you get rationing a la Zeke Emanuel and then you have no monetary barrier to care but a bureaucratic barrier to care.
I see the situation as a spectrum with 100% guaranteed coverage at one end with hideous inefficiencies and eventual rationing, vs a totally free market at the other where some people are unable to afford care. What we’re really arguing about is where we want to sit on that line. Do you want them to lack care due to cost or due to government bureaucracy?
If you think this can’t happen, consider the case of a man who lives (maybe “lived” by now) in Sweden . He had cancer and the Swedish health care system denied him the drug his doctor recommended. He offered to pay for it himself. They said he couldn’t do that because it wouldn’t be fair to others who weren’t as wealthy. Yes, the country of Sweden said a man couldn’t use his private property to save his own life.
The U.S. has nothing close to a free market in healthcare, especially when you look at how much certain industries and the government control it.
Doctor, you correctly observe that most people believe that we cannot have a health care system that does not include third party payers and rigid regulatory control of charges to the public.
Regulations and laws are necessary to protect the public from unfair money making schemes by some groups of doctors, not you. For example, Medicare and many states have curtailed or banned the practice of balance billing in which a patient is billed for an exorbitant balance by an out of network doctor or medical practice that refuses to be satisfied with the customary fee offered by the insurer.
Some may feel that it is unfair to deny the doctor’s right to negotiate his/her own fee. But there is no negotiation. Often the balance is due to the fact that the primary in network surgeon is surreptitiously assisted by an out of network doctor who bills for an amount that is not just a little more, but several times more than the primary surgeon has agreed to accept, eg., $4000 for the surgeon and $40,000 for the assistant.
Other times the balance is a result of the fact that an in network hospital’s bill does not include out of network emergency doctors’ bills because the doctors are undisclosed outside contractors and no longer employed by the hospital.
We need a single payer system. Our current insurance system already contains rationing because if you can’t afford the co pay you can’t go to the doctor. My son needs to see an orthopedic doctor and it will be weeks before I can afford to take him. He only takes cash and checks and won’t bill me for the co pay. So I am already experiencing rationing and have been for years, and I have insurance.
Sorry to hear about your son, Petunia.
Countries with single-payer systems always have rationing built into their system. In France, for example, you have to get permission before certain procedures are done. A few years ago, the mother of a friend of mine was denied a complete knee replacement. After a lot of wrangling that too many months and lots of back-and-forth mail (yup), she got a partial replacement done. Partial because it was cheaper, apparently.
It’s always the same. There is nothing on this planet that isn’t rationed in some form or fashion, either through price, or through long waits, or whatever. Nothing of value is available in unlimited quantity.